






High-volume hospitals face a relentless operational challenge: thousands of appointments moving through a system that was never designed for today's patient loads. When scheduling breaks down, the consequences ripple outward longer wait times, burned-out staff, lost revenue, and patients who simply don't come back. A properly engineered hospital scheduling system doesn't just manage appointments; it orchestrates people, resources, and data in real time, at scale.
This guide draws on production-grade architecture decisions, proven algorithms, and real-world implementation patterns to help healthcare CIOs, product heads, and engineering leaders build scheduling infrastructure that holds up under pressure.
Why Traditional Scheduling Fails at Scale
Most hospitals didn't start with a scheduling problem. They started with a spreadsheet, then a calendar tool, then a bolt-on module from their EHR vendor. By the time patient volume grows to thousands of daily appointments, these systems are held together with workarounds.
The core failure modes are consistent across institutions:
No-show rates between 20–30% in outpatient settings leave expensive slots empty while waitlists grow. Without predictive modeling, administrators react after the fact rather than managing proactively.
Fragmented resource booking means a physician's calendar, an imaging machine's availability, and a procedure room's schedule are managed in separate systems with no shared awareness. The result is a doctor ready, a room booked, and no equipment or vice versa.
Peak-hour collisions between scheduled visits and emergency walk-ins overwhelm the front desk and clinical staff simultaneously, with no intelligent triage or overflow routing.
Integration debt compounds everything. Legacy EHRs, billing platforms, and lab systems exchange data through point-to-point connections that break when any one system updates.
These aren't process problems. They're architecture problems and they require engineering solutions.
What a Modern Patient Scheduling System Must Actually Do
Before designing anything, it helps to be precise about requirements. For a facility processing 5,000 or more daily appointments, the system needs to operate across several dimensions simultaneously.
A patient scheduling system at enterprise scale must coordinate physicians, nurses, rooms, equipment, and labs as a unified resource pool not as separate calendars. A cancellation in one area should automatically trigger reallocation across all dependencies.
It must handle real-time state changes. A cancellation, an emergency admission, or a late-running procedure should propagate through the schedule in seconds, not when someone manually updates a spreadsheet.
Patients increasingly expect consumer-grade self-service: mobile booking, multilingual interfaces, SMS and push reminders, and the ability to reschedule without calling a front desk. These aren't nice-to-haves in competitive US healthcare markets they directly affect patient acquisition and retention.
On the operational side, administrators need dashboards that surface utilization rates (target: 85–90%), flag emerging bottlenecks, and forecast demand well enough to staff appropriately.
| Requirement Area | Core Capabilities | Target Metrics |
|---|---|---|
| Scalability | Horizontal scaling, auto-sharding | 10,000+ concurrent users; sub-500ms response |
| Integration | FHIR-compliant EHR/EMR APIs, telehealth, billing | RESTful + HL7 standards |
| Security | AES-256 encryption, role-based access control | HIPAA-compliant; full audit logging |
| Reliability | Failover clustering, redundant infrastructure | 99.99% uptime SLA |
System Architecture: Why Microservices Are the Right Foundation
The architectural decision that determines everything else is whether to build on a monolithic or microservices foundation. For high-volume hospital environments, this isn't a close call.
A monolithic hospital appointment scheduling system fails in predictable ways: a spike in booking requests slows the entire application; a bug in the notification module can take down scheduling; scaling requires replicating the entire application even if only one component is under load.
Microservices solve these problems by decomposing the system into independently deployable, independently scalable services. The core modules for a hospital scheduling platform include:
Scheduling Engine: slot allocation logic, conflict detection, optimization
Patient Portal: web and mobile booking interfaces
Notification Service: SMS, email, and push via Twilio or AWS SNS
Analytics Engine: ML-driven demand forecasting and utilization reporting
Integration Layer: EHR, billing, and telehealth API connectors
These services communicate through an API gateway (Kong or Envoy) and an event bus (Apache Kafka) for asynchronous operations. The data layer separates concerns: PostgreSQL for transactional slot data, Redis for high-speed caching of availability queries, and MongoDB for audit logs and unstructured records.
Deployment runs on Kubernetes (AWS EKS or Azure AKS), enabling auto-scaling based on real metrics CPU utilization above 70%, queue depth above 100 rather than scheduled capacity windows. This architecture scales linearly: doubling traffic requires adding pods, not redesigning systems.
This kind of infrastructure-level thinking is what separates a software product development engagement from a simple feature build. The architecture decisions made early determine whether the system handles a 3x surge on flu season or collapses under it.
The Algorithms That Eliminate Scheduling Bottlenecks
The scheduling engine is where the real engineering work happens. Rule-based systems "book the next available slot" work at low volume. They create bottlenecks at scale.
Slot Optimization with Genetic Algorithms
Scheduling across 10 physicians, 200 available slots, multiple room types, and shared equipment is an NP-hard combinatorial optimization problem. Genetic algorithms handle this class of problem well.
The approach treats each possible schedule configuration as an individual in a population. A fitness function evaluates each configuration against weighted objectives:
f = w₁ · utilization + w₂ · wait_time⁻¹ + w₃ · no_show_probability
Crossover operations swap slot assignments between configurations; mutation operators introduce small variations. Over successive generations, the algorithm converges on configurations that maximize utilization while minimizing wait times. On GPU-accelerated clusters, convergence for a 200-slot daily schedule completes in under five seconds fast enough for real-time rescheduling when disruptions occur.
Real-Time Queue Management for the Hospital Queue Management System
Walk-ins and emergencies require a different approach: a priority queue implemented on Redis Sorted Sets. Each patient receives a score based on arrival timestamp and clinical priority:
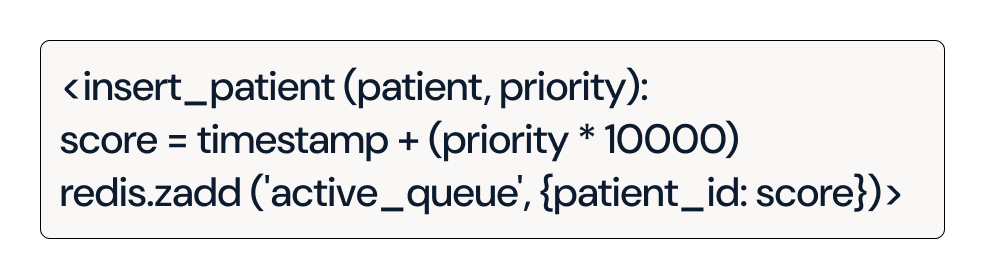
This gives the hospital queue management system O(log n) insertion and retrieval performance at any volume. Priority tiers map to clinical urgency emergencies at P0, chronic condition follow-ups at P1, routine visits at P2 with tunable weights to prevent systematic unfairness at lower priority levels.
Predictive No-Show Modeling
No-show prediction is where the system shifts from reactive to proactive. XGBoost models trained on historical appointment data incorporating patient demographics, appointment lead time, day of week, distance to facility, and even local weather conditions via external APIs can predict no-show probability with approximately 85% accuracy.
The output drives overbooking strategy: if predicted no-show probability for a slot is p, the system books at capacity 1/(1−p). A 20% predicted no-show rate justifies booking 1.25 patients per slot filling the slot without systematically overbooking.
| Algorithm | Application | Accuracy / Performance |
|---|---|---|
| Genetic Algorithm | Daily schedule optimization | Converges in <5s on GPU clusters |
| Priority Queue | Walk-in and emergency handling | O(log n) operations |
| XGBoost | No-show prediction and overbooking | ~85% prediction accuracy |
These algorithms combined power a medical appointment scheduling software that responds to conditions rather than just following rules.
End-to-End Patient Flow: From Booking to Post-Visit
The patient journey through the scheduling system should be seamless from the first interaction to the last. Here's how a well-designed patient flow management system handles it:
Patient Inquiry: Patient accesses the portal via mobile or web. Availability is served from Redis cache, returning results in milliseconds.
Slot Proposal: The scheduling engine queries available slots, runs the GA optimization, and proposes the best fit based on patient history, physician specialization, and resource availability.
Confirmation and OTP: Patient confirms via one-time password. The booking event is published to Kafka, triggering downstream services synchronously.
Automated Reminders: 24-hour and 1-hour reminders dispatched via the notification service. Reminder cadence and channel (SMS, email, push) are personalized based on patient preference data a function of product design and prototyping work validated through A/B testing.
Check-in: QR code scan at arrival integrates directly with the clinic scheduling system, updating queue position and triggering room assignment.
Post-Visit Feedback: Satisfaction data feeds back into the ML models, continuously improving no-show prediction and slot optimization.
When the system encounters overload conditions a surge of walk-ins during peak hours, for example patients are automatically diverted to virtual queue positions or offered telehealth alternatives, preventing front-desk collapse.
HIPAA Compliance and Security Architecture
Healthcare scheduling systems in the United States handle Protected Health Information (PHI) at every touchpoint. This is not an area where compliance can be treated as an afterthought.
The security architecture must address PHI at multiple layers. Data at rest is encrypted with AES-256. Data in transit uses TLS 1.3 across all service-to-service and client-to-server communication. Role-based access control (RBAC) limits data exposure to the minimum necessary for each role scheduling staff see appointment data; they don't see clinical notes.
A zero-trust security model implemented through an identity provider like Okta ensures that no service or user is implicitly trusted, even within the internal network. Every request is authenticated and authorized explicitly.
Audit logging captures every data access event who accessed what, when, and from where meeting HIPAA's audit control requirements (45 CFR § 164.312(b)). Logs are immutable and retained according to applicable state and federal requirements.
US healthcare organizations are also navigating increasing state-level privacy regulations alongside federal HIPAA requirements. The system architecture should support configurable data residency and retention policies to accommodate this regulatory diversity.
Regular penetration testing and SOC 2 Type II certification are baseline expectations for any enterprise healthcare software deployment in the US market.
Integration with US Healthcare Ecosystems
A clinic scheduling system that can't integrate with existing clinical infrastructure creates more problems than it solves. US hospitals are predominantly built around Epic and Cerner EHR platforms, with HL7 FHIR as the interoperability standard mandated by the 21st Century Cures Act.
The integration layer should expose FHIR-compliant APIs for bidirectional data exchange with EHR systems pulling patient history, insurance verification, and prior authorization data into the scheduling workflow, and pushing appointment confirmations and check-in events back to the clinical record.
Billing integration with systems like Athenahealth or Waystar should support real-time eligibility verification at the point of scheduling, reducing claim denials downstream. Telehealth integration (Zoom for Healthcare, Microsoft Teams for Healthcare) should be native, not bolted on a patient who can't make an in-person appointment should be able to convert to a telehealth visit in one step.
API contract testing (Pact) and mock environments (Postman) during development prevent integration failures from propagating to production.
Cloud and DevOps Engineering for Zero-Downtime Operations
The most sophisticated scheduling algorithms provide no value if the system is unavailable during peak booking hours. Cloud and DevOps engineering discipline is what converts architectural intent into operational reliability.
Containerized microservices deployed on Kubernetes enable rolling updates with zero downtime new versions are deployed incrementally while traffic is gradually shifted, with automatic rollback if error rates increase. CI/CD pipelines (GitHub Actions or GitLab CI) enforce automated testing gates before any deployment reaches production.
Observability infrastructure Prometheus for metrics, Grafana for visualization, Jaeger for distributed tracing provides the visibility needed to identify performance degradation before it becomes user-facing downtime. Alerts fire on latency increases, error rate spikes, or queue depth growth before they affect patients.
Infrastructure as Code (Terraform) ensures environments are reproducible and change controlled. Service mesh (Istio) manages traffic routing, circuit breaking, and mutual TLS between services. Chaos engineering (Gremlin) validates that the system recovers gracefully from simulated failures a critical step before go-live at a facility where downtime directly impacts patient care.
| Practice | Tool | Operational Benefit |
|---|---|---|
| Infrastructure as Code | Terraform | Reproducible, auditable environments |
| Service Mesh | Istio | Traffic control, observability, mTLS |
| Chaos Engineering | Gremlin | Validated resilience under failure |
| Auto-scaling | Kubernetes HPA | Handles 3x surge without intervention |
UI/UX Design: Where Adoption Is Won or Lost
The best-engineered backend is invisible to patients. What they experience is the interface. Product strategy & consulting informs design decisions that directly affect scheduling adoption rates and patient satisfaction scores.
For patients, the priority is friction elimination: mobile-first design, intuitive calendar views, and a booking flow completable in under three minutes. Accessibility compliance (WCAG 2.1) is both a legal requirement under the ADA and a practical necessity for serving elderly patients who represent a disproportionate share of hospital visits.
For clinical staff, the priority is situational awareness: utilization heatmaps, real-time queue status, and alert surfaces for schedule disruptions. Staff who can see the full picture respond faster and make better decisions.
Personalization features AI-driven slot suggestions based on a patient's appointment history, preferred providers, and stated preferences demonstrably improve booking completion rates. One US hospital system reported a 40% increase in self-scheduling adoption after implementing personalized slot recommendations combined with gamified reminder engagement.
Prototype testing and iterative refinement through product design and prototyping cycles before development investment reduces redesign costs and produces interfaces that actually match how clinical workflows operate.
Real-World Case Studies
Urban Multi-Specialty Hospital System
A 1,200-bed multi-specialty facility processing 4,500 daily appointments was experiencing frequent peak-hour system crashes, a 28% no-show rate, and average wait times of 45 minutes. The hospital engaged a product engineering services team to rebuild its scheduling infrastructure on a microservices architecture deployed on AWS, with GA-based optimization and XGBoost no-show prediction.
Eighteen months post-implementation:
| Metric | Before | After |
|---|---|---|
| Daily Appointments Processed | 4,500 | 6,200 |
| No-Show Rate | 28% | 12% |
| Average Wait Time | 45 minutes | 29 minutes |
| System Uptime During Peak | Frequent crashes | 99.9% |
| Resource Utilization | ~68% | 92% |
The ROI was measurable within 12 months through slot efficiency gains alone, before accounting for improved patient retention.
Rural Clinic Network with Connectivity Constraints
A network of rural clinics faced a different challenge: intermittent internet connectivity made cloud-dependent systems unreliable. The solution was a healthcare scheduling software built as an offline-first Progressive Web Application (PWA) appointments booked locally, synced when connectivity restored. IoT-enabled queue sensors fed real-time occupancy data into the hospital queue management system, reducing walk-in processing time by 50% without requiring consistent connectivity.
AI and the Future of Hospital Scheduling
The current generation of scheduling systems optimizes within known constraints. The next generation anticipates constraints before they materialize.
Large language model integration enables conversational booking: "Schedule a cardiology follow-up for next Tuesday afternoon, and check if my usual parking space is available" becomes a single natural-language interaction rather than a multi-step form flow. Early implementations using GPT-4 class models in HIPAA-compliant deployments show patient satisfaction improvements among elderly populations who find form-based interfaces challenging.
Multimodal models that process clinical notes, imaging schedules, and surgical calendars simultaneously can identify scheduling conflicts that no rule engine would catch a post-surgical follow-up scheduled before discharge imaging is complete, for example.
Public health data integration influenza surveillance, regional COVID-19 case counts, local event calendars feeds predictive models that anticipate volume surges 2–3 weeks out, allowing proactive staffing and slot release decisions rather than reactive crisis management.
Blockchain-based audit trails for scheduling events provide tamper-evident records suitable for malpractice litigation and regulatory examination an increasingly relevant capability as US healthcare organizations face growing legal scrutiny.
Implementation Roadmap and Investment Framework
Successful deployments follow a phased approach that delivers value quickly while building toward full capability.
Phase 1 Foundation (Months 1–3) Core booking engine, basic EHR integration, patient portal MVP, and HIPAA-compliant infrastructure. This phase is sufficient to eliminate the most acute bottlenecks and establish the data collection baseline for ML models.
Phase 2 Intelligence (Months 4–9) No-show prediction, GA-based optimization, telehealth integration, and multi-site support. The analytics dashboard becomes operational, surfacing utilization data that informs staffing and capacity decisions.
Phase 3 Continuous Optimization (Ongoing) Model retraining on accumulated data, UX refinement based on usage patterns, integration with emerging health data sources, and capability expansion as clinical workflows evolve.
Investment Range: $500K–$2M for enterprise implementations, depending on existing infrastructure, integration complexity, and scope. ROI typically materializes within 12 months through direct efficiency gains reduced no-shows, higher slot utilization, and reduced administrative labor before accounting for patient retention and satisfaction improvements.
The key to staying within scope and timeline is engaging experienced product engineering services partners early in the process, during product strategy & consulting and architecture phases, before development investment is committed. Decisions made in the first 90 days determine whether the system scales to meet the hospital's five-year growth trajectory or requires a costly rebuild at scale.
Frequently Asked Questions
What is the typical implementation timeline for a hospital scheduling system?
For a facility processing 3,000–7,000 daily appointments, a production-ready core system typically requires 3–4 months. Full AI-driven optimization and multi-site support adds another 3–6 months. Total timelines depend heavily on EHR integration complexity and existing infrastructure.
How does an AI-powered scheduling system handle HIPAA compliance?
Compliant implementations use AES-256 encryption at rest, TLS 1.3 in transit, RBAC for access control, and immutable audit logging. All AI model training on PHI occurs in HIPAA Business Associate Agreement (BAA)-covered environments, with de-identification protocols where applicable.
What's the ROI case for replacing legacy scheduling systems?
Primary ROI drivers include reduced no-show rates (industry benchmarks show 15–20% improvement with predictive overbooking), increased slot utilization (from typical 65–70% to 85–90%), reduced administrative labor through self-service booking, and improved patient retention through better experience.
Can the system integrate with Epic and Cerner?
Yes, through FHIR R4-compliant APIs. Both Epic and Cerner support FHIR-based third-party integrations. The integration scope read-only patient data versus full bidirectional clinical data exchange affects complexity and timeline.
What happens to scheduling data during a system outage?
Properly engineered systems use event sourcing with Kafka to ensure no scheduling events are lost during partial outages. Offline-capable patient portals queue bookings locally and sync when connectivity restores. Failover clustering maintains availability even when individual nodes fail.
How long does staff training typically take?
For clinical and administrative staff using the scheduling interface, typical training cycles are 4–8 hours for core functions. System administrators managing configuration and integrations require 2–3 days of structured training. Well-designed interfaces built on user research significantly reduce time-to-competency.
Building a hospital appointment scheduling system that performs reliably at scale is a systems engineering challenge as much as a software one. The facilities that get this right with sound architecture, intelligent algorithms, rigorous security, and continuous optimization see measurable returns in operational efficiency, patient satisfaction, and revenue performance. The ones that patch legacy systems together continue absorbing the costs of bottlenecks indefinitely.
Design High-Volume Healthcare Systems with Experts




