






Emergency departments are drowning in wait times. The average patient spends 2.5 hours in limbo before seeing a doctor and in many urban hospitals, that number stretches past four hours during peak periods. Hospital administrators know the problem. They've seen the data on hospital capacity planning failures, the overcrowded waiting rooms, and the staff burnout that follows. What they often miss is this: throwing machine learning at the problem without fixing the underlying system is like adding a faster engine to a car with no transmission.
The real breakthrough in emergency department patient flow doesn't come from predictive algorithms alone. It comes from engineering systems that connect every touchpoint in the patient journey from the moment someone books an appointment to when a bed opens up for the next admission. This is where product engineering services become the difference between a 20% improvement that plateaus in six months and a 40% reduction in wait times that compounds over years.
This article is written for hospital operations leaders, CIOs, and digital health product owners who are already using scheduling or AI tools but still see long ER wait times. We'll break down why ML-only approaches fail, what actually works in modern hospital queue management systems, and how strategic product engineering creates sustainable patient flow improvements that executives can measure.
The Real Problem: Why Your Scheduling Software Isn't Working
Walk into any hospital leadership meeting about wait times, and you'll hear the same pattern: "We implemented an AI scheduling tool six months ago. It worked initially no-shows dropped 15%. But now we're back where we started, and the emergency department is still backed up."
The issue isn't the technology. It's that these tools optimize one part of a multi-stage system. A hospital management system might predict which patients will show up, but if there's no bed available when they arrive, or if discharge processes take three hours instead of one, the prediction becomes irrelevant. You've optimized the front door while the hallway remains jammed.
This is where Product Strategy & Consulting enters the equation. Before hospitals deploy any technology, they need to map their actual patient flow not the idealized version in a process document, but the messy reality of how patients move through the system today. That mapping reveals where the real constraints live, and more importantly, which constraints can be engineered away versus which ones require operational change.
Problem #1: Data Silos Break Real-Time Patient Flow
Why it fails: Queue tools fail because real-time system integration doesn't exist across EHR, beds, and scheduling.
What works: Product engineering services that create real-time integration layers across systems.
Most hospitals run 15-20 separate systems that don't communicate. Your EHR knows patient history. Your scheduling system knows appointments. Your bed management system knows availability. Your radiology system knows imaging slots. But none of them talk to each other in real time.
What this looks like in practice:
A patient arrives for an appointment at 2 PM. The scheduling system shows them as "checked in." But the bed management system doesn't know a bed just opened up on the third floor. The doctor finishes seeing another patient and waits 15 minutes before someone manually checks bed availability. The patient who could have been admitted immediately sits in the waiting room for 45 minutes because two systems couldn't share one piece of information.
The engineering solution:
Custom integration layers that connect disparate systems through FHIR and HL7 APIs. One regional hospital built middleware that synchronizes bed status, appointment schedules, and treatment room availability every 30 seconds. When a bed opens, the system automatically alerts the next patient in queue and notifies the admitting physician.
Result: Wait times for bed assignments dropped from 78 minutes to 22 minutes not because they added beds, but because they eliminated the communication delay between systems.
Engineering effort: 8-12 weeks for middleware development, 4 weeks for testing and rollout
Organizational change: Required buy-in from IT, clinical operations, and bed management teams
Problem #2: Legacy Systems That Can't Be Replaced
Why it fails: Modern queue software assumes control over all scheduling, but legacy systems operate in isolation.
What works: API wrappers that expose legacy data without touching old code.
Here's the uncomfortable truth: that 15-year-old radiology scheduling system isn't going anywhere. It's embedded too deeply. The radiologists know it. Staff are trained on it. And the risk of migration losing historical data, retraining 200 people, potential system downtime is too high for most hospital boards to approve.
What breaks because of this:
Modern queue management software assumes it can control all scheduling. But when radiology runs on a separate legacy system, the queue management tool has no visibility into imaging appointments. Patients get scheduled for consultations before their imaging results are ready. Doctors wait for reports that haven't been generated yet. The entire flow stalls because one system operates in isolation.
The engineering solution:
Build around the legacy system instead of replacing it. One hospital's product engineering team created an API wrapper that sits on top of their old radiology platform. The wrapper exposes scheduling data to the modern queue management system without touching the legacy code. Radiologists continue using their familiar interface. The queue system gets real-time visibility.
Result: Total development time: 6 weeks. Migration risk: zero. Radiology appointment visibility improved from 0% to 100%.
This approach wrapping legacy systems rather than replacing them is a core capability of Software Product Development teams who understand healthcare IT constraints. You're not just building new features; you're building bridges between old and new infrastructure.
Problem #3: Discharge Delays That Nobody Measures
Why it fails: Emergency departments don't have a bed shortage they have a discharge bottleneck.
What works: Automated parallel-processing workflows that trigger multiple discharge steps simultaneously.
Patients who could go home sit in inpatient beds for hours waiting for discharge paperwork, prescriptions, transportation arrangements, and follow-up appointments. Every hour of discharge delay is an hour the emergency department can't admit someone new.
What this looks like in practice:
A patient is medically cleared for discharge at 9 AM. The discharge order sits in the physician's queue until 10:30 AM. Pharmacy receives the prescription order at 11 AM but the medication isn't ready until 12:30 PM. Transportation is called at 1 PM but the patient doesn't leave until 3 PM. Six hours of bed occupancy after medical clearance and every one of those hours blocks an admission from the emergency department.
The engineering solution:
Automated discharge workflows that trigger parallel processes instead of sequential handoffs. When a physician enters a discharge order, the system simultaneously:
Routes prescription orders to pharmacy with priority flagging
Notifies case management to arrange follow-up appointments
Alerts transportation services to prepare for pickup
Generates discharge instructions and insurance paperwork
Result: One health system using this parallel-processing approach cut average discharge time from 4.2 hours to 1.8 hours. The result: 30% improvement in emergency department patient flow because inpatient beds became available faster. No new beds were built. No staff were added. The engineering fixed the process bottleneck.
Engineering effort: 10-14 weeks for workflow automation development
Organizational change: Required coordination between physicians, pharmacy, case management, and transport services
This is the kind of workflow automation that Product Design and Prototyping teams can model and test before full deployment running simulations to identify which parallel processes will have the highest impact on bed turnover rates.
Problem #4: No-Shows Create Cascading Capacity Waste
Why it fails: ML predicts no-shows but doesn't automatically reallocate wasted slots.
What works: Dynamic slot reallocation with automated waitlist management that acts on predictions.
When a patient doesn't show up for their appointment, most systems leave the slot empty. That's 20-30 minutes of physician time wasted. Multiply that by 5-10 no-shows per day, and you've lost 2-3 hours of capacity which means other patients wait longer, which increases frustration, which increases future no-shows.
What breaks the typical ML solution:
Predictive models can tell you which patients are likely to miss appointments. But prediction without action doesn't fix anything. If the system predicts a 70% no-show probability for Patient A's 2 PM slot, what happens next? In most deployments: nothing. The slot stays reserved until 2 PM, then it's too late to fill it.
The engineering solution:
Dynamic slot reallocation with automated waitlist management. When the system predicts a high no-show probability 24 hours in advance, it:
Sends automated confirmation requests to the patient
If no response within 4 hours, places the slot in a "provisional" state
Notifies waitlisted patients that a slot may open
If original patient confirms, the slot is secured
If original patient doesn't respond by 12 hours before appointment, the slot automatically transfers to the highest-priority waitlist patient
Result: One clinic implemented this approach and reduced no-show impact from 12% lost capacity to 3% lost capacity. They didn't eliminate no-shows they eliminated the wasted slots that no-shows create.
Engineering effort: 6-8 weeks for slot reallocation logic and patient notification system
Organizational change: Required staff training on provisional slot management and patient communication protocols
This is appointment scheduling optimization through engineering, not just through better predictions.
If your hospital already uses AI tools but still sees long wait times, the issue is likely architectural not predictive. The bottleneck isn't prediction accuracy it's system integration and workflow automation.
The Four-Stage Patient Flow That Actually Matters
If you want to understand why queue management best practices differ so dramatically from generic ML solutions, follow a single patient through the actual system:
Stage 1: Pre-Arrival Booking
Before the patient ever walks in, effective systems send appointment confirmations, automated reminders, and allow easy rescheduling via SMS or app. This isn't about prediction it's about making it frictionless for patients to update their availability. Dynamic slot reallocation means if someone cancels at 2 PM, the system immediately offers that slot to a waitlisted patient.
Stage 2: Digital Check-In
Walk-ins and scheduled appointments converge at this point. Self-service kiosks and mobile check-in handle insurance verification, consent forms, and initial triage questions. One major health system reported 75% faster check-ins after deploying AI-enabled kiosks but the win wasn't the AI, it was the workflow redesign that eliminated paper forms and reduced front-desk bottlenecks.
Stage 3: Real-Time Queue Adjustment
This is where most systems fail. A patient checks in for a routine visit, but the doctor discovers something that requires imaging. Now the patient needs a slot in radiology, which bumps another scheduled case, which delays a specialist consult, which holds up a bed assignment. The best hospital queue management systems don't just track where patients are they adjust downstream queues based on treatment progress.
Stage 4: Discharge Coordination
Inpatient beds don't free up when treatment ends they free up when discharge paperwork clears, transportation is arranged, prescriptions are filled, and follow-up appointments are scheduled. Hospitals that engineer this process see dramatic improvements because beds turn over faster.
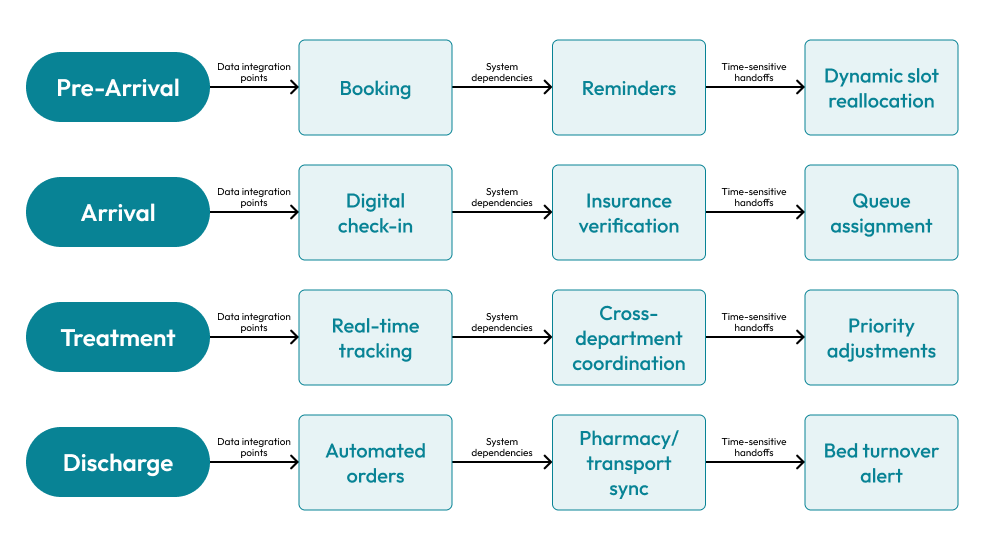
Each arrow should show: Data integration points, System dependencies, Time-sensitive handoffs
Hybrid Queue Systems Reduce ER Wait Times by 25% More Than ML-Only Tools
Why it works: Hybrid systems pair ML predictions with engineered workflows that execute actions automatically.
What it requires: Integration between forecasting models and operational systems.
The most effective hospital queue management deployments combine predictive analytics with operational redesign. This isn't about choosing between technology and process it's about using each where it has the highest leverage.
| Approach | Core Mechanism | Wait Time Reduction | Sustainability | Best Use Case |
|---|---|---|---|---|
| ML-Only | Demand forecasting, slot optimization | 20–30% initially, plateaus at 6–9 months | Low (doesn't address root causes) | Single-department scheduling |
| Rule-Based Systems | Fixed triage protocols, static allocation | 10–15% | Medium (reliable but inflexible) | Low-variability clinics |
| Hybrid (ML + Process) | Predictive models + dynamic workflows | 38–45% sustained over 18+ months | High (adapts to change) | Multi-department hospital systems |
| Integrated QMS | Virtual queues, feedback loops, real-time coordination | Up to 50% in pilot programs | Highest (requires ongoing tuning) | Health systems with EHR integration |
The hybrid advantage comes from pairing ML's strengths (pattern detection, probabilistic ranking) with engineered workflows that respond to those predictions. For example, if ML forecasts a 40% surge in respiratory cases due to flu season, the hybrid system doesn't just alert administrators it automatically:
Adjusts staffing schedules based on predicted case types
Pre-allocates isolation rooms for infectious patients
Notifies suppliers to stock additional respiratory supplies
Shifts elective procedures to off-peak hours
This level of coordination requires Software Product Development that connects forecasting models to operational systems. It's not a dashboard showing predictions it's an integrated platform that turns predictions into executable actions.
Capacity Planning: Managing Resource Allocation Without Waste
Why it matters: Hospital capacity planning determines whether predictions translate into better patient flow.
What works: Coordinated strategies that balance staff, beds, and equipment against demand patterns.
Here's a truth that doesn't fit on vendor slide decks: capacity planning is harder than building ML models, and it matters more.
Capacity strategy breaks into four modes, and hospitals need all four simultaneously:
Lead Capacity: Adding staff and resources ahead of predictable surges (flu season, summer trauma spikes). This requires financial planning, hiring timelines, and the political will to staff for peaks rather than averages.
Lag Capacity: Reactive expansion post-surge. Cheaper in the short term but leads to perpetual firefighting. Most hospitals default here because budgets favor known costs over speculative staffing.
Match Capacity: Real-time flexing based on current demand. Cross-trained staff who can shift between departments, flex rooms that convert from observation to inpatient beds, dynamic scheduling that adjusts in four-hour blocks.
Adjustment Capacity: Daily predictive modeling that fine-tunes resource allocation. This is where ML helps not as the whole solution, but as one input into a broader planning process.
The hospitals seeing 40%+ improvements in emergency department patient flow aren't using one strategy they're orchestrating all four. They use predictive models to trigger lead capacity decisions, match capacity to handle daily variability, lag capacity for unexpected events, and adjustment protocols to optimize continuously.
This orchestration is fundamentally an engineering problem. It requires Cloud and DevOps Engineering to ensure systems remain reliable during surges, real-time data pipelines that don't fail under load, and monitoring dashboards that surface capacity constraints before they become crises. One regional health system built a centralized command center that pulls data from EHRs, bed management, staffing systems, and transport logistics into a single view. They can see system-wide bottlenecks in real time and reroute resources accordingly.
| Strategy | Description | Implementation Complexity | Best For |
|---|---|---|---|
| Lead Capacity | Pre-add staff/resources before predictable surges | Medium (requires forecasting) | Seasonal patterns (flu season) |
| Lag Capacity | React after demand spike occurs | Low (but creates delays) | Budget-constrained operations |
| Match Capacity | Real-time resource adjustment | High (requires automation) | Daily variability management |
| Adjustment Capacity | Continuous predictive optimization | High (requires ML + automation) | High-volume emergency departments |
When to Talk to a Product Engineering Team (Not Another Vendor)
Why product engineering matters: Queue bottlenecks are architectural problems, not software feature gaps.
When it's needed: When integration, compliance, and workflow complexity exceed vendor capabilities.
If your hospital is experiencing persistent queue bottlenecks despite deploying scheduling software or predictive tools, the issue is likely architectural. This is the moment when Product Design and Prototyping becomes critical not to build yet another standalone tool, but to redesign how systems interact.
Product engineering enters the equation when:
Integration complexity exceeds tool capabilities: Your EHR, billing system, lab equipment, and scheduling platform don't communicate. You need custom APIs, data transformation layers, and real-time sync protocols work that vendors don't scope because it's specific to your environment.
Compliance requirements block standard solutions: Data protection regulations mean you can't just pipe patient data through third-party ML platforms. You need federated learning models, on-premise deployment, or hybrid architectures that keep sensitive data within your network.
Workflows don't match software assumptions: Off-the-shelf queue systems assume linear patient journeys (check-in → triage → treatment → discharge). But your emergency department handles simultaneous treatment streams, where a single patient might occupy three queues concurrently (waiting for lab results while holding a treatment room while queued for imaging). Standard software breaks under this complexity.
Legacy systems can't be replaced: That 15-year-old radiology scheduling system isn't going anywhere it's embedded too deeply, and migration risk is too high. You need Product Strategy & Consulting to figure out how to build around it rather than replace it.
Real example:
In one public hospital deployment, a product engineering team tackled discharge delays caused by fragmented communication between physicians, pharmacy, and transport. They didn't build a new hospital management system they built a lightweight integration layer that sat between existing tools, automated medication reconciliation, and triggered transport requests when discharge orders cleared.
Result: Wait times dropped 30% in the first quarter because bed turnover accelerated. The engineering insight wasn't sophisticated AI it was recognizing that the bottleneck was a coordination problem, not a prediction problem.
Engineering effort: 10 weeks for integration layer development
Organizational change: Required coordination between clinical, pharmacy, and operations teams
Real-World Outcomes: What Works Beyond the Hype
One major health system deployed an AI scheduling system that reduced appointment booking time from 4-20 hours to 15 minutes. Impressive, but the real gain came from the operational change that accompanied it: instead of requiring phone calls and manual calendar checks, patients could self-schedule through a mobile app integrated with the EHR. The AI handled slot optimization, but the engineering made it accessible and automated.
A pharmacy chain in the Middle East implemented WhatsApp-based virtual queuing. Patients received real-time updates on wait times and could arrive exactly when needed. Lobby congestion dropped 60% because people stopped physically waiting. This wasn't ML it was appointment scheduling optimization through a messaging interface that met patients where they already were.
One government health ministry rolled out a digital hospital queue management system across multiple facilities. The platform integrated self-service check-in kiosks, real-time queue displays, and mobile notifications. Patients could track their position remotely and receive alerts when to arrive for their turn. The system didn't predict demand—it managed demand more transparently, which reduced perceived wait times and actual congestion simultaneously.
The pattern across successful deployments: technology enablement paired with workflow redesign. ML contributed, but it wasn't the hero. The hero was the engineering team that mapped patient journeys, identified friction points, and built integrated systems that addressed root causes rather than symptoms.
The Engineering That ML Can't Do Alone
Why engineering matters: Queue systems succeed by solving integration, compliance, and adaptation simultaneously not by improving predictions.
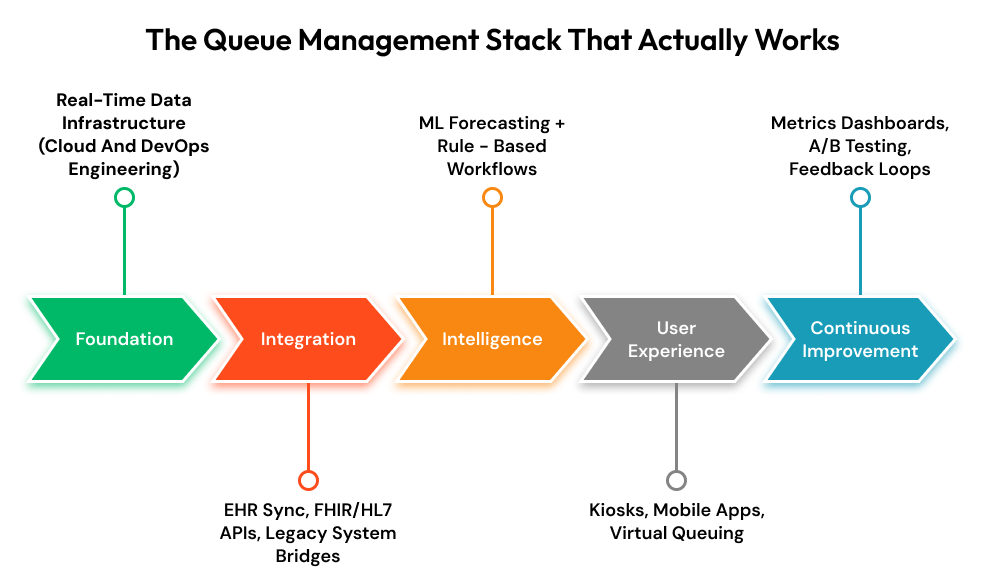
Modern hospital queue management systems succeed when they solve three problems simultaneously: integration, compliance, and adaptation.
Integration: Healthcare IT environments are notoriously fragmented. EHRs don't natively sync with legacy scheduling platforms, radiology systems, or billing software. FHIR and HL7 standards help, but implementation requires custom engineering to handle data transformations, error handling, and real-time updates across disparate systems. This is where Software Product Development teams build the connective tissue APIs, middleware, and sync protocols that make isolated tools function as a unified platform.
Compliance: Data protection violations carry severe penalties. Any system handling patient data needs encryption at rest and in transit, audit logs, role-based access controls, and data residency guarantees. Hospitals can't just deploy cloud-based ML platforms without custom security architectures that meet regulatory requirements. Product engineering teams design these architectures deciding what data stays on-premise, what can move to cloud, and how to federate learning models across distributed environments without centralizing sensitive information.
Adaptation: Patient flow patterns change. New treatments emerge, regulations shift, payer requirements evolve. A hospital management system built five years ago might not account for telehealth integrations or remote monitoring workflows that became standard during recent health crises. Systems need to be architected for change modular, API-driven, with clear separation between business logic and data models. This isn't about building everything from scratch; it's about choosing the right abstraction layers so future changes don't require full rewrites.
Real example:
One health system partnered with a product engineering team to redesign their patient tracking system. Instead of a monolithic application, they built a microservices architecture where each department (emergency, radiology, inpatient) could update their module independently. When new imaging equipment arrived with different scheduling protocols, only the radiology service needed modification the rest of the system continued functioning.
Result: This architectural choice, made during Product Design and Prototyping, saved 18 months of rework compared to their previous system.
Engineering effort: 16-20 weeks for microservices architecture design and implementation
Organizational change: Required IT governance changes to support independent module updates
7 Signs Your Queue Problem Is Architectural, Not Algorithmic
If your hospital experiences 3 or more of these, you need product engineering not better AI:
Data silos: Your EHR, scheduling, and bed management systems don't share real-time data
Manual workarounds: Staff regularly call other departments to check availability instead of viewing it in the system
Discharge delays: Average discharge time exceeds 3 hours after medical clearance
No-show waste: Empty appointment slots aren't automatically reallocated to waitlist patients
Legacy dependencies: Critical systems are 10+ years old and can't be replaced
Integration gaps: New tools require manual data entry because they don't connect to existing systems
Workflow mismatches: Your patient flow doesn't match the linear assumptions of off-the-shelf software
If this describes your hospital, the next step isn't another scheduling tool it's an architectural assessment.
What Hospitals Should Demand from Their Next Queue Management Project
If you're evaluating solutions, here's the shift in thinking that separates incremental improvements from transformational ones:
Stop asking: "What can this tool predict?"
Start asking: "How does this integrate with our existing workflows and systems?"
Stop asking: "What's the ROI based on vendor case studies?"
Start asking: "What specific bottleneck in our patient flow will this address, and how will we measure improvement?"
Stop asking: "Can we deploy this in 90 days?"
Start asking: "What operational changes need to happen alongside this technology for it to deliver sustained results?"
The hospitals achieving 40-50% reductions in wait times aren't buying products they're commissioning product engineering services tailored to their environment. They're working with teams that understand both healthcare workflows and modern software architecture. They're treating queue management best practices as a system design problem, not a vendor selection problem.
Final Thought: Systems Over Silver Bullets
The emergency waiting room will never be empty. Healthcare demand is inherently unpredictable, resources are finite, and emergencies don't schedule themselves. But the difference between a 2.5-hour wait and a 90-minute wait is profound for patient outcomes, staff morale, and hospital financials.
That difference doesn't come from deploying the latest AI model. It comes from hospitals brave enough to treat queue management best practices as an engineering discipline one that requires integration expertise, compliance rigor, workflow redesign, and the humility to acknowledge that technology alone can't fix systemic problems.
Machine learning has a role. But it's one component in a much larger architecture. The hospitals that understand this distinction are the ones already seeing results. The ones still chasing algorithmic silver bullets will keep experiencing the same plateau: initial excitement, modest gains, and eventual stagnation.
The question isn't whether to use ML. It's whether you're engineering a system that can actually leverage it.





