







Author's Note: Having worked alongside engineering teams building platforms for healthcare chains spanning 50+ locations, one pattern emerges repeatedly: the most expensive decisions aren't made during scale they're made at day one, before the first patient record is ever written.
Across healthcare platforms we've worked on, over 70% required architectural rework between locations 5–10 not because of bad engineering, but because of early design assumptions that were never questioned.
Why 5 Locations Is the Breaking Point
Most teams assume scaling problems appear gradually. They don't. They arrive all at once and almost always around location five.
Here's why that number is so consistent across healthcare platform builds:
At 1–2 locations, systems operate in isolation. Each site functions independently, and shared infrastructure feels like a convenience, not a requirement. At 3–4 locations, shared workflows begin to overlap scheduling conflicts emerge, reporting requests multiply, and teams start stitching together manual workarounds. At 5 or more locations, three things happen simultaneously:
Cross-location reporting becomes mandatory for operations and compliance
Scheduling conflicts increase exponentially as shared availability pools grow
Compliance auditing shifts from locally managed to centrally required
This is the point where monolithic assumptions fail not gradually, but all at once. The engineering team that handled four locations with patches suddenly faces problems that patches can't solve.
If you don't design for this inflection point early, you'll end up redesigning your platform under pressure later.
Most teams don't fail because they scale too fast they fail because their architecture assumes they won't.
The Multi-Location Problem Nobody Talks About Early Enough
The biggest risk in healthcare platform development isn't a bad feature it's a good product built on the wrong foundation.
Most healthcare technology teams begin with a single clinic. The architecture reflects that a monolithic codebase, a single database, hardcoded location logic. It works. Until it doesn't.
When the organization opens a second branch, the engineering team patches. Third branch, more patches. By the fifth location, the platform has accumulated enough technical debt to slow every new feature by weeks. Data lives in silos. Compliance reporting becomes a manual nightmare. The product that once felt nimble now feels like concrete.
This is the hidden cost of not designing for multi-location healthcare system design from day one. And in healthcare where uptime, data integrity, and regulatory compliance are non-negotiable the consequences go beyond engineering inconvenience. They affect patient care.
Quick Check: Is Your Platform Ready for Multi-Location Scale?
The biggest mistake teams make is assuming their single-location architecture will hold. Run this self-assessment if you answer "yes" to two or more, your architecture is already limiting your growth:
Adding a new location requires code changes, not just configuration
Reporting across locations is slow, inconsistent, or done manually
Patient data is difficult to access or reconcile across branches
A deployment at one location affects all others simultaneously
Compliance audits require significant manual effort to prepare for
Most teams wait too long to fix this making it 3–5x more expensive when they finally do. If two or more of these apply, the cost of inaction is already compounding with every new branch you open.
When You Actually Need This Architecture (and When You Don't)
The right architecture depends entirely on where you are in your growth curve and over-engineering too early is as costly as under-engineering too late.
| Locations | Reality | What You Need |
|---|---|---|
| 1–2 | Simple systems work fine | Solid monolith with clean data models |
| 3–5 | Early strain begins scheduling, reporting, data sync | Start planning multi-tenancy; separate core domains |
| 5–10 | Architecture becomes the bottleneck | Microservices, event-driven design, tenant isolation |
| 10+ | Must redesign or accept compounding cost | Full scalable healthcare platform architecture |
Most teams hit serious problems between locations three and five not because they built badly, but because they built for where they were, not where they were going. The inflection point almost always arrives faster than expected.
Why Multi-Location Architecture is Fundamentally Different in Healthcare
Healthcare platforms must balance centralized access with strict data isolation and this dual constraint is what makes multi-location healthcare system design categorically different from other SaaS domains.
A retail chain opening new locations shares inventory logic. A healthcare chain shares patient histories, clinical workflows, appointment systems, EMR records, and insurance billing all governed by HIPAA in the US, GDPR in Europe, and a patchwork of local regulations elsewhere.
This means healthcare app development teams face a constraint almost no other domain faces at the same intensity: systems must be centralized enough to provide a unified patient view, and isolated enough to ensure one location's data never bleeds into another's. Getting this balance wrong doesn't just create engineering problems it creates compliance violations, patient safety risks, and legal exposure.
Key Insight Most healthcare platforms don't fail at scale they slow down first. By the time issues become clearly visible (typically after 5–10 locations), fixing them requires re-architecting core systems, not simply adding features. The window to design this right is always earlier than teams expect.
Monolith vs. Microservices: The Decision That Defines Your Ceiling
The biggest architectural decision in healthcare platform development isn't which database to use it's whether to build for independent scaling from day one.
| Approach | Short-Term | Long-Term | Best For |
|---|---|---|---|
| Monolith | Faster MVP, simpler deployment | Breaks at scale; expensive to refactor | 1–3 location platforms |
| Modular Monolith | Moderate speed, better structure | Easier to decompose later | Early-stage with clear growth plans |
| Microservices | Slower start, more infra overhead | Scales cleanly; independent deployments | 5+ location scalable healthcare systems |
| Event-Driven Microservices | Highest initial investment | Most resilient; best for compliance | Enterprise hospital management system for multiple branches |
The choice isn't about which is "better" it's about which one your growth curve actually demands. Most teams that get this wrong choose a monolith for speed, then spend 18 months paying down architectural debt when location four or five arrives.
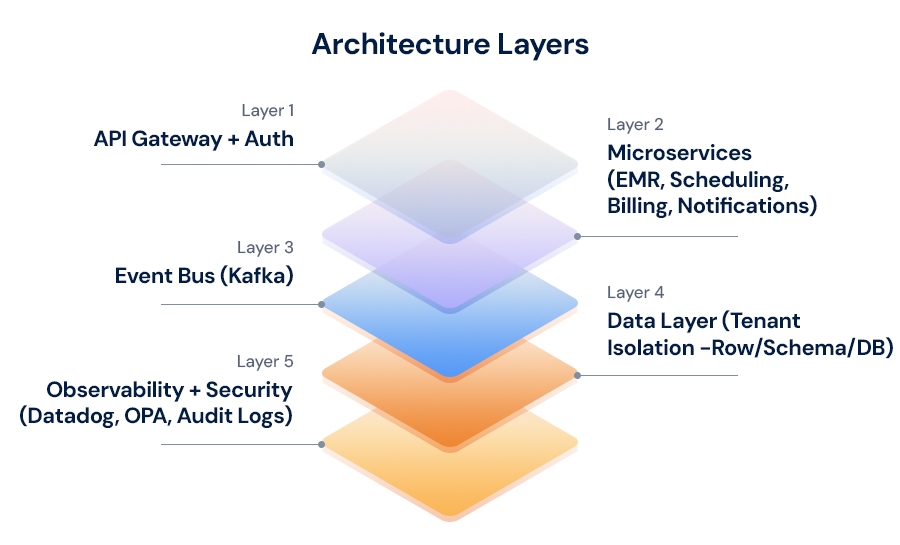
The Five Architectural Pillars Every Scalable Healthcare Platform Needs
The difference between a platform that scales and one that fractures comes down to five decisions made before the first line of production code.
1. Multi-Tenancy: The Hardest Decision to Reverse
Multi-tenancy is the single most important architectural decision and the hardest to fix later. A multi-tenant healthcare application model, where locations share infrastructure with strictly isolated data, is the foundation everything else depends on. The three models each fit different scale points:
Row-level isolation: Cost-effective for smaller multi-clinic management systems, but complex to query safely as tenant count grows
Schema-per-tenant: Strong isolation with moderate overhead the right starting point for most healthcare software for multi-location clinics
Database-per-tenant: Compliance gold standard, highest operational cost preferred for enterprise deployments
This choice is nearly impossible to reverse cleanly once real patient data exists. It must be made before application code is written.
💡 Key Insight: 40–60% of "location-specific" logic teams assume needs custom handling is actually standardizable. One clinic chain we worked with discovered that 11 of their 18 "branch-specific" billing rules were identical across locations they had simply never been mapped against each other. Identifying this early dramatically simplifies your tenant model and reduces ongoing maintenance cost.
2. Domain-Driven Microservices: Scale What Needs Scaling
The biggest mistake in healthcare software architecture is building one service that handles everything. Separate your platform into domain-driven services: patient management system, appointment scheduling, billing, notifications, and analytics. Each scales independently. During flu season, your scheduling service needs 10x capacity your billing service does not.
3. Event-Driven Communication: Eliminate Cascading Failures
In a distributed healthcare platform development environment, synchronous API calls create fragility if one service slows, everything downstream slows with it. Event buses like Apache Kafka decouple services, enabling eventual consistency while maintaining resilience. A patient discharge event at one branch simultaneously triggers billing, inventory restocking, and follow-up scheduling independently and auditably.
4. Cloud-Native Infrastructure: Provision Branches in Hours, Not Weeks
Cloud-based healthcare software built on auto-scaling groups, multi-region deployments, and infrastructure-as-code (Terraform) means a new branch becomes a configuration change, not a multi-week engineering project. This is what scalable cloud architecture for healthcare actually delivers in practice not just elasticity, but operational speed.
5. Zero-Trust Security: Compliance Built In, Not Bolted On
Every service-to-service call is authenticated. Every data access is logged. Policy engines like OPA (Open Policy Agent) enforce at the policy layer not the application layer that a user at Branch A can never access Branch B records. This is what healthcare SaaS architecture requires to pass compliance audits without engineering heroics.
Process Flow: From Single-Site MVP to Multi-Location Platform
The teams that scale successfully don't move faster they sequence decisions better.
Phase 1 Audit and Requirements Mapping: Before writing code, map your actual workflows. Which processes are identical across locations? Which are genuinely location-specific? Teams working with product engineering consulting partners routinely find that 40–60% of assumed location-specific logic is standardizable. The product design and prototyping phase is where this discovery pays the most dividends.
Phase 2 Design the Tenant Model: Choose your multi-tenancy approach before building anything else. Define how tenant IDs propagate through your API layer, how they're enforced at the database level, and how your architecture handles cross-tenant reporting which administrators always eventually need, regardless of what they say at project kickoff.
Phase 3 Build Core Services as Isolated Modules: Your patient management system, appointment engine, and EMR core should be built as independent services from the start even if they initially run on shared infrastructure. Isolation at the code level costs almost nothing now; isolation retrofitted later costs months.
Phase 4 Implement Healthcare Integration Systems: Building your integrations on FHIR/HL7 standards from day one means connections with third-party EHRs, lab systems, insurance providers, and telehealth platforms are repeatable across locations not rebuilt from scratch for each new branch.
Phase 5 Progressive Multi-Location Rollout: Validate the multi-tenant model at two or three locations before regional expansion. Healthcare devops best practices blue-green deployments, feature flags, canary releases ensure a problematic release doesn't simultaneously impact every branch.
Building the EMR and Scheduling Core for Scale
The EMR system architecture is where most healthcare platforms make their most consequential and most expensive technical mistakes.
CQRS (Command Query Responsibility Segregation) consistently outperforms simpler patterns at scale. Patient record creation and updates flow through a command pipeline validated, event-sourced, written to Kafka. Read operations draw from purpose-built models: MongoDB for unstructured clinical notes, PostgreSQL for structured records, Elasticsearch for cross-location search. This separation means high-volume reads never compete with write operations keeping patient data current.
For the appointment scheduling system, temporal workflow engines like Temporal.io handle multi-location complexity far better than traditional state machines. Here's what getting this wrong looks like in practice: one clinic chain we worked with had scheduling logic hardcoded per location. Adding a new branch required 14 code changes across 6 services, a full QA cycle, and a coordinated deployment taking an average of 3 weeks per new location. After moving to a configuration-driven scheduling model, new locations were onboarded in under 48 hours without a single code change.
💡 Key Insight: Healthcare workflow automation at the scheduling layer reduces no-show rates by 25–35% and cuts administrative time by 40–60% compared to manual systems. These gains compound as location count grows.
Cloud and DevOps Foundation for Healthcare Infrastructure Scalability
Most healthcare infrastructure scalability failures aren't architecture failures they're operational failures that good DevOps practices would have caught.
Key practices that separate platforms that handle growth from ones that don't:
Infrastructure as Code via Terraform a new location's infrastructure should be a configuration change, not a manual provisioning project
Blue-green deployments for zero-downtime releases across all locations simultaneously
Chaos engineering using tools like Gremlin to validate that redundancy actually works before a real failure exposes it to patients
Global observability through Datadog or Prometheus + Grafana, giving teams a unified health view across every branch from a single dashboard
💡 Key Insight: Data gravity is the most underestimated healthcare infrastructure scalability challenge. As each location accumulates years of patient records, moving or replicating that data becomes exponentially harder. Multi-region replication designed in from the start costs a fraction of what retrofitting it costs at location fifteen.
Common Mistakes Teams Make When Scaling Healthcare Software
The most expensive scaling mistakes in healthcare aren't technical failures they're design decisions that seemed reasonable at one location and catastrophic at ten.
Hardcoding location logic is the most common. When branch-specific rules live in application code rather than configuration, adding a location requires code changes, testing cycles, and full deployments. Every value that varies by location scheduling templates, notification content, billing codes should live in a configuration service, not in conditional logic.
Ignoring eventual consistency implications causes subtle data bugs that are extremely difficult to debug in production. In a distributed centralized healthcare system architecture, different services will temporarily hold different views of the same data. This is acceptable if designed for; it's catastrophic if assumed away.
Underinvesting in tenant isolation creates security debt that compounds quickly. Row-level security implemented only at the application layer is one middleware bug away from a data breach. Database-level row security policies, enforced independently of application code, provide the compliance-grade protection that auditors increasingly require.
Treating compliance as a phase is perhaps the most expensive mistake of all. HIPAA audit logging, GDPR data residency requirements, and SOC 2 controls are dramatically cheaper to build in than to retrofit into a system already serving live patients across multiple locations.
When to Use Product Engineering Services (and What They Actually Solve)
The question isn't whether you need external expertise it's whether you catch the architecture gaps before or after they become expensive.
Most healthcare organizations have deep clinical domain expertise. Fewer have the engineering depth to make architectural decisions correctly under launch timeline pressure. Product engineering services for healthcare platforms accelerate outcomes because experienced teams bring pattern recognition from multiple builds knowing that a schema-per-tenant model working well at five locations typically shows stress between fifteen and twenty, and designing the migration path before it becomes urgent.
The right product engineering consulting partners engagement solves three things your internal team often can't prioritize under delivery pressure:
Architecture clarity What to build vs. refactor, sequenced correctly for your growth stage
Operational scalability Cloud and DevOps engineering practices that make platforms maintainable at scale, not just at launch
Early risk visibility Observability and system insights that surface problems before your patients experience them
For teams at the beginning of this journey, engagements that start with architecture audits consistently deliver higher ROI than engagements that start with feature delivery because they eliminate the rework that would otherwise consume 30–50% of future engineering capacity.
What a Healthcare Architecture Engagement Actually Looks Like
A typical healthcare platform architecture engagement runs in three stages and the value is front-loaded in the first two weeks, not at the end.
Weeks 1–2 Architecture Audit: Map the current system, identify tenant model gaps, document location-specific logic, and quantify the cost of inaction across your planned growth trajectory. Most teams are surprised by what this surfaces.
Weeks 3–6 Blueprint and Roadmap: Design the target architecture, prioritize refactoring vs. rebuild decisions, and define the migration path that keeps the platform live throughout the transition.
Month 2 onward Phased Implementation: Execute against the roadmap in prioritized phases, with early phases focused on the highest-risk components typically tenant isolation and data model changes first.
Teams that complete this process typically reduce new location onboarding time from 6–8 weeks to under 5 days, and reduce per-location infrastructure cost by 40–55%.
How to Avoid Rebuilding Your Healthcare Platform in Two Years
The platforms that require full rebuilds at year two all share one thing: they solved the right problems for the wrong scale.
The healthcare platforms being built today will need to support capabilities just emerging: AI-assisted clinical documentation, predictive scheduling based on population health data, edge computing for remote clinic locations, and real-time interoperability across provider networks. Each capability is dramatically easier to add to a healthcare software architecture built on modular, event-driven, cloud-native foundations.
The investment in scalable healthcare systems design isn't just about handling ten locations instead of one. It's about keeping your architectural optionality intact ensuring that a new capability in year three is a feature addition, not a platform rebuild.
FAQs: Multi-Location Healthcare Platform Architecture
Before you make architectural decisions, here are the most common questions teams ask at this stage:
Should we rebuild or refactor our existing healthcare platform?
This depends on where you are in your growth curve. Under 5 locations, targeted refactoring with a clear architectural direction is usually sufficient. Between 5–10 locations, a hybrid approach using the strangler fig pattern gradually replacing monolithic modules with independent services typically works best. Beyond 10 locations, a partial rebuild of core systems, particularly tenant isolation and data models, is often unavoidable. The key is honest assessment of your current debt, not optimism about what patches can hold.
What is the best architecture for multi-location healthcare platforms?
A multi-tenant, cloud-native architecture with domain-based microservices and event-driven communication is the most scalable approach. The specific tenancy model row-level, schema-per-tenant, or database-per-tenant depends on compliance requirements and growth trajectory. Most healthcare software for multi-location clinics starts with schema-per-tenant and migrates as regulatory pressure increases.
When should a healthcare platform move to multi-tenancy?
From day one, ideally. Retrofitting multi-tenancy after real patient data exists is complex, risky, and expensive. The data model changes required touch nearly every layer of the system and typically take 3–6 months of focused engineering effort to execute safely.
How many locations can a monolithic healthcare system handle before breaking?
Most monolithic systems show meaningful scaling issues between 3–5 locations, particularly in scheduling conflicts, cross-location reporting, and data consistency. Problems are typically manageable at five locations and critical by fifteen.
What are the biggest risks when scaling healthcare platforms?
Hardcoded location logic, weak tenant isolation at the database level, underinvestment in compliance infrastructure, and treating eventual consistency as a defect rather than a design constraint. These four issues account for the majority of scaling failures in healthcare platform development.
How much does it cost to get multi-location architecture wrong?
Architectural rework on a live healthcare platform costs 30–50% of the original build cost, plus opportunity cost from slowed feature delivery during the rework period. For platforms serving 10+ locations, this regularly exceeds $500K in engineering cost alone.
How long does it take to redesign a healthcare platform for multi-location scale?
A structured architecture redesign takes 6–12 weeks for planning and prototyping, depending on existing technical debt. The planning phase is where most value is created implementation timelines vary based on how incrementally the migration can be executed.
Can existing healthcare systems be upgraded without a full rebuild?
Yes. Strangler fig patterns where new services gradually replace monolithic modules work well for healthcare platforms where downtime is unacceptable. Tenant isolation and data model changes must come before service decomposition.
What compliance requirements most affect multi-location healthcare architecture?
HIPAA mandates encryption at rest (AES-256), encryption in transit (TLS 1.3), strict audit logging, and data access controls. GDPR adds data residency requirements that affect where patient data can physically reside. Both are significantly cheaper to architect for than to retrofit.
Start With the Architecture, Not the Feature List
The teams that build healthcare platforms successfully at scale share one discipline: they resist the pressure to start with features and instead start with the architectural decisions that make features sustainable.
If you're planning a multi-clinic management system, evaluating a hospital management system for multiple branches, or rebuilding a platform showing the strain of unplanned growth the right time to address architecture is before the next location goes live, not after it.
Will your platform break at 5 locations? Get a clear answer →
In 30 minutes, we'll show you where your architecture sits, what's at risk at your next growth stage, and what fixing it actually costs. No sales pitch just clarity on where you stand and what it takes to scale sustainably.
Because at scale, architecture decisions aren't technical choices they're business risks.
Find out what breaks at five locations




