







Most telemedicine platforms do not fail because of a bad idea. They fail because the technical foundation was not built to handle real-world conditions unpredictable user growth, complex compliance requirements, and the daily workflows of actual doctors and patients. Most failures are not product problems they are engineering and architecture problems.
If you are a founder, product head, or CTO planning to build or scale a telemedicine product, this blog breaks down why telehealth apps fail after launch and what structured product engineering does to prevent it.
What Is a Telemedicine Platform?
A telemedicine platform is a digital system that enables remote healthcare delivery through video consultations, patient data management, scheduling, billing, and integrations with clinical systems like EHR and EMR. It connects patients and providers across devices, locations, and healthcare networks and when the underlying architecture is weak, every one of those connections becomes a failure point.
Why Telemedicine Platforms Fail After Launch (Common Telehealth Challenges)
Most telemedicine platforms fail due to preventable engineering decisions not market demand. Industry studies estimate that up to 75% of digital health platform failures trace back to architecture, compliance, and integration mistakes made in the first few months of development.
Key Insight: Industry studies estimate that up to 75% of telemedicine platform failures come from preventable engineering and planning mistakes not market demand or funding.
Many teams rush to ship an MVP, hit early traction, and assume the hard part is over. Then, 12 to 18 months later, the cracks appear. Video calls drop during peak hours, doctors complain about switching between five tools, a compliance audit flags missing encryption, and the cost to fix everything is two to three times the original build budget.
A hospital managing 200 daily appointments can lose 50 or more sessions per day from dropped video calls alone during peak hours a direct hit to provider trust and patient retention. Most teams do not fail because they lack features they fail because their system cannot support growth. This is the default outcome when telemedicine app development skips the foundational work.
What This Means for Your Business
Poor telemedicine engineering decisions create four direct business consequences: delayed launches, user churn, compliance exposure, and expensive rebuilds.
Delayed launches mean lost market opportunity in a window that competitors fill quickly
Poor user experience directly reduces patient retention if a video call lags or onboarding takes more than three minutes, users leave and do not return
Compliance failures create legal exposure, potential fines, and loss of payer relationships
Rebuild costs for a poorly architected platform typically range from $40K–$100K for a partial rebuild to $150K–$300K for a full overhaul, plus 6–12 months of lost development time
The business case for getting this right early is not just about quality it is about survival. Most teams do not realize the full cost of poor early decisions until they are already paying to undo them. Most of these risks can be identified and resolved early with a structured architecture review before they become expensive mid-lifecycle problems.

The Four Root Causes Behind Telemedicine Platform Challenges Teams Overlook
Telemedicine platforms fail due to four core issues: architecture, compliance, integrations, and UX. Each one compounds the others, and ignoring any single layer creates cascading problems at scale.
Weak architecture that cannot scale
Telehealth scalability issues almost always trace back to the same decision: building a monolithic system in the early stages. One large codebase handling video, billing, scheduling, and records together works fine at 500 users. At 50,000, it becomes a liability. Any spike in usage can crash the entire system, not just one feature. Healthcare app development done properly uses microservices from the start, isolating video streaming, authentication, payments, and notifications into independent modules that scale separately without affecting each other.
To understand why this matters, here is the practical difference between the two approaches:
Monolith vs. Microservices in Telemedicine
Monolith: Faster initial build, lower upfront cost, but carries high long-term risk one failure point can bring down the entire platform
Microservices: Slightly slower start, but independently scalable, resilient under load, and far easier to maintain as the platform grows
Compliance treated as an afterthought
HIPAA telemedicine architecture is not a layer you add at the end it is a foundational design requirement. Platforms that add encryption, access controls, and audit logging as retrofits spend far more time and money than those that embed these standards into the original design. For platforms operating across borders, GDPR adds another compliance layer that requires separate data handling logic entirely. Missing these requirements does not just create legal risk it destroys user trust at the exact moment you need to build it. Most of these compliance gaps can be identified early with a structured architecture review before development begins.
No integration with existing clinical workflows
Doctors will not adopt a platform that forces them to manually transfer patient data from their EHR system. Patients will not trust a platform that cannot sync with pharmacy systems or lab results. Healthcare software development that ignores FHIR and HL7 integration standards forces providers to manage parallel systems, which accelerates abandonment. This is one of the most common reasons why technically functional platforms still fail in the market.
UX designed for engineers, not users
Elderly patients need large fonts, clear navigation, and offline-capable interfaces. Doctors need EHR data visible inside the consultation screen without switching tabs. When design decisions are made by engineers optimizing for build speed rather than clinical workflows, the result is a technically correct product that no one wants to use. A 5-second load time alone can cause a 25% drop in user engagement during the critical onboarding phase.
Failure Impact at a Glance
| Failure Area | Business Impact | Common Example |
|---|---|---|
| Poor UX/UI | 25% user drop-off | Laggy video, confusing navigation |
| No scalability | Crashes during surges | Monolithic backend, no load balancing |
| Integration gaps | Provider abandonment | No EHR sync, manual data entry |
| Compliance issues | Legal risk, fines | Missing HIPAA encryption |
| Over-reliance on AI | Loss of trust | No human fallback in triage flow |
How Product Engineering Solves This
Product engineering reduces telemedicine failure risk by addressing architecture, compliance, integrations, and UX before development begins not after the first major incident.
The difference between platforms that survive and those that get rebuilt in year two comes down to when structure enters the process. Cloud and DevOps Engineering, Software Product Development, and Product Strategy and Consulting services built on a product engineering foundation follow a deliberate sequence rather than a reactive one.
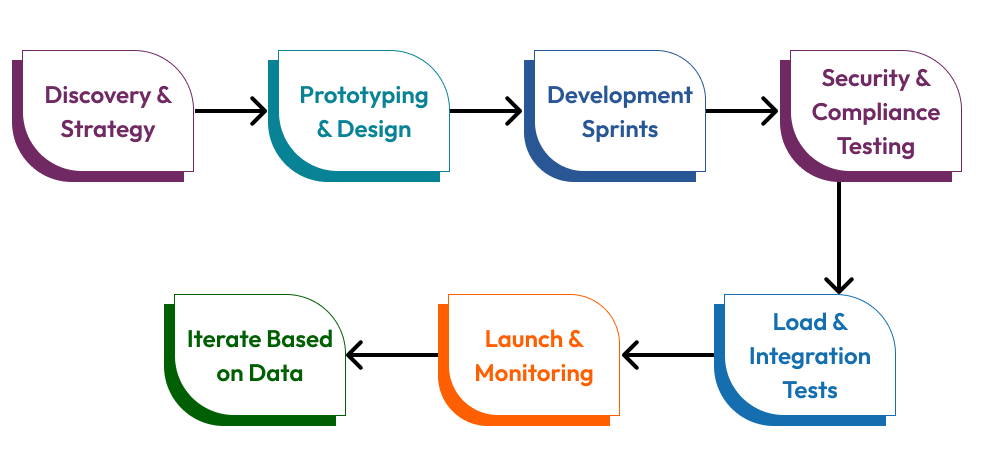
The process starts with a discovery phase that maps actual clinical workflows, identifies compliance requirements specific to the target market, defines integration priorities, and stress-tests assumptions before a single line of code is written. This phase alone eliminates a large category of post-launch problems that most teams only discover under real traffic.
Design and prototyping follow, with real users both patients and providers testing interactions before development begins. This is where accessibility requirements, onboarding flows, and doctor dashboard designs get validated against real behavior. The goal is not a beautiful prototype; it is evidence that the product will actually be used.
Development runs in Agile sprints with compliance requirements embedded into each module. Telemedicine software development built this way treats HIPAA controls, end-to-end encryption (TLS 1.3), and role-based access controls as core features not optional additions to be reviewed before launch. Testing includes load simulations, security audits, and usability sessions with real clinical teams. Most teams skip this phase to hit a launch date. The teams that skip it are the ones spending $200K on rebuilds 18 months later.
The Architecture That Actually Works
A scalable telemedicine platform architecture requires five core components and getting any one of them wrong creates system-wide risk.
Frontend: React Native for cross-platform healthcare mobile app development, ensuring consistent experience across iOS and Android without duplicating codebases
Backend: Node.js or Go microservices, each responsible for a single domain video, auth, scheduling, billing so issues in one module do not cascade across the system
Data layer: Encrypted PostgreSQL for structured clinical data, Redis for caching high-frequency reads, all configured to HIPAA standards from the ground up
Integration layer: FHIR-compliant APIs for EHR/EMR connectivity, pharmacy APIs for e-prescriptions, and IoT endpoints for wearable device data
Infrastructure: Kubernetes for container orchestration and auto-scaling, CDN for low-latency global video delivery, Prometheus and Grafana for real-time monitoring
This stack reflects what platforms like Teladoc have built to handle millions of consultations reliably deep EHR integration, insurer connectivity, and telemedicine platform development infrastructure that scales without manual intervention. Healthcare application development services that build on this foundation from day one avoid the single most expensive mistake in the industry: retrofitting compliance and scalability into a system that was never designed for them.
When Should You Invest in Product Engineering?
The right time to invest depends on where your platform currently stands. The earlier the investment, the lower the cost and the lower the risk.
Pre-MVP stage: Define your architecture blueprint, compliance scope, and integration requirements before writing a single line of code this is where you prevent 80% of future problems
Post-MVP (0–10K users): Validate scalability assumptions, run load tests, and identify telehealth software challenges and integration gaps before growth exposes them
Growth stage (10K+ users): Focus on compliance optimization, EHR integration depth, and healthcare platform scalability tuning to support scale without system instability
Each stage has a different risk profile and a different cost of inaction. Waiting until problems appear is almost always the most expensive approach. Healthcare software scalability issues that cost $20K to fix at the architecture stage routinely cost $150K or more to fix after launch.
Early Warning Signs You Are Already Facing This Problem
The following indicators suggest architectural debt is already building inside your platform:
Feature releases are taking longer with each sprint, even though team size has not changed
Engineering spends more time fixing bugs than shipping new capabilities
Doctors are using workarounds copy-pasting data between systems, keeping separate notes outside the platform
Load testing has never been run on the production environment
Compliance was reviewed once at launch and has not been revisited since
These are not minor inefficiencies. They are early indicators of systemic architectural debt that compounds with every new user and every new feature added on top of a fragile foundation.
Cost of Poor Telemedicine Engineering Decisions
Poor telemedicine engineering decisions do not show up immediately they compound quietly until a rebuild becomes unavoidable. The real numbers behind delayed action:
Partial rebuild: $40K–$100K, typically needed 12–18 months post-launch
Full platform rebuild: $150K–$300K, triggered by compliance failure or infrastructure collapse
Time cost: 6–12 months of stalled product development during reconstruction
Market cost: Competitors who built correctly during this window do not give that ground back
Most teams discover these issues only after launch when fixing them is 2–3x more expensive than addressing them early. Investing in structured custom healthcare software development from the start discovery, architecture review, compliance-first design, integration planning costs a fraction of what reactive fixes demand.
Telehealth platform architecture is not just a software problem. It is a product strategy problem, a compliance problem, and a clinical workflow problem simultaneously. The teams that treat it as all three from day one are the ones still growing three years after launch.
What You Should Do Next
If you are in the planning phase, the single highest-leverage action is an architecture review before development begins. Map your integration requirements, define your compliance scope, and validate your scaling assumptions with real load projections not optimistic guesses.
If you are post-launch and recognizing the early warning signs above, a structured audit of your current telehealth app development foundation will surface the highest-risk areas before they become rebuild-level problems.
If you are unsure where your platform stands, most teams benefit from a 30-minute architecture review before making further product investments. It is the fastest way to get clarity on risk, cost, and priority without committing to a full engagement.
Frequently Asked Questions
Why do telemedicine platforms fail after launch?
Most failures are caused by poor architecture decisions made early in development not by lack of features or market demand. Weak scalability, missing HIPAA compliance, absent EHR integrations, and poor UX design are the four root causes that account for the majority of post-launch failures.
How much does it cost to rebuild a telemedicine platform?
Partial rebuilds typically cost between $40K and $100K and are usually needed 12 to 18 months after launch. Full platform rebuilds range from $150K to $300K, often triggered by a compliance failure or infrastructure collapse. The time cost 6 to 12 months of stalled development is often more damaging than the financial cost.
What is the most important factor in telemedicine platform success?
A scalable, compliance-first architecture that integrates with existing healthcare systems from day one. Platforms that build HIPAA controls, EHR connectivity, and microservices-based infrastructure into the original design consistently outperform those that treat these as secondary concerns.
When should a company invest in product engineering for telemedicine?
The earlier, the better. Pre-MVP investment in architecture and compliance planning prevents the majority of post-launch problems. For teams already live, a structured architecture audit at the 0–10K user stage is the most cost-effective intervention before growth exposes underlying weaknesses.
What does a product engineering approach look like for healthcare platforms?
It follows a structured sequence: discovery and workflow mapping, design and prototyping with real users, Agile development with compliance embedded at each sprint, load and security testing before launch, and continuous monitoring post-launch. This approach combining Product Strategy and Consulting, Cloud and DevOps Engineering, and AI-driven healthcare product development is what separates platforms that scale from those that rebuild.
Strengthen your telemedicine platform




