







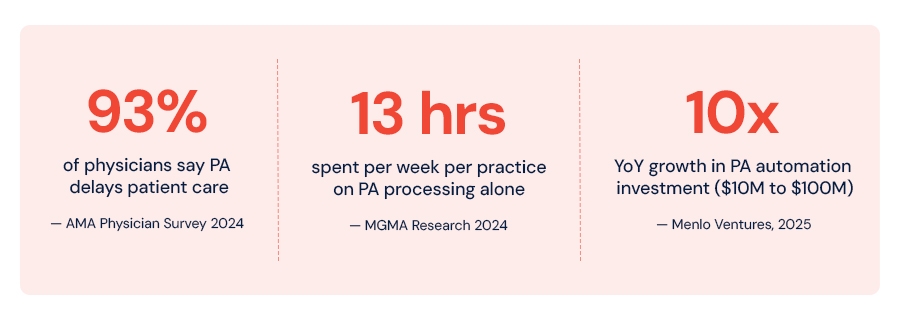
A physician orders a biologic infusion for a rheumatoid arthritis patient. Before treatment can begin, the practice must submit a prior authorization request to the payer, wait two to five days for a response and, in nearly one in four cases, receive a denial that triggers an entirely separate appeals process. The physician's office has 38 other requests queued behind this one.
This is not a hypothetical. It is the operational reality for hundreds of thousands of U.S. healthcare providers every week, making prior authorization automation one of the fastest-growing areas of healthcare workflow automation today.
Prior authorization was originally designed as a clinical guardrail a mechanism to ensure expensive or risky treatments were medically necessary before payers committed to covering them. What it has become is something different: a friction-generating administrative layer that costs the healthcare system billions of dollars annually, delays care for millions of patients, and consumes a disproportionate share of clinical and operational staff capacity.
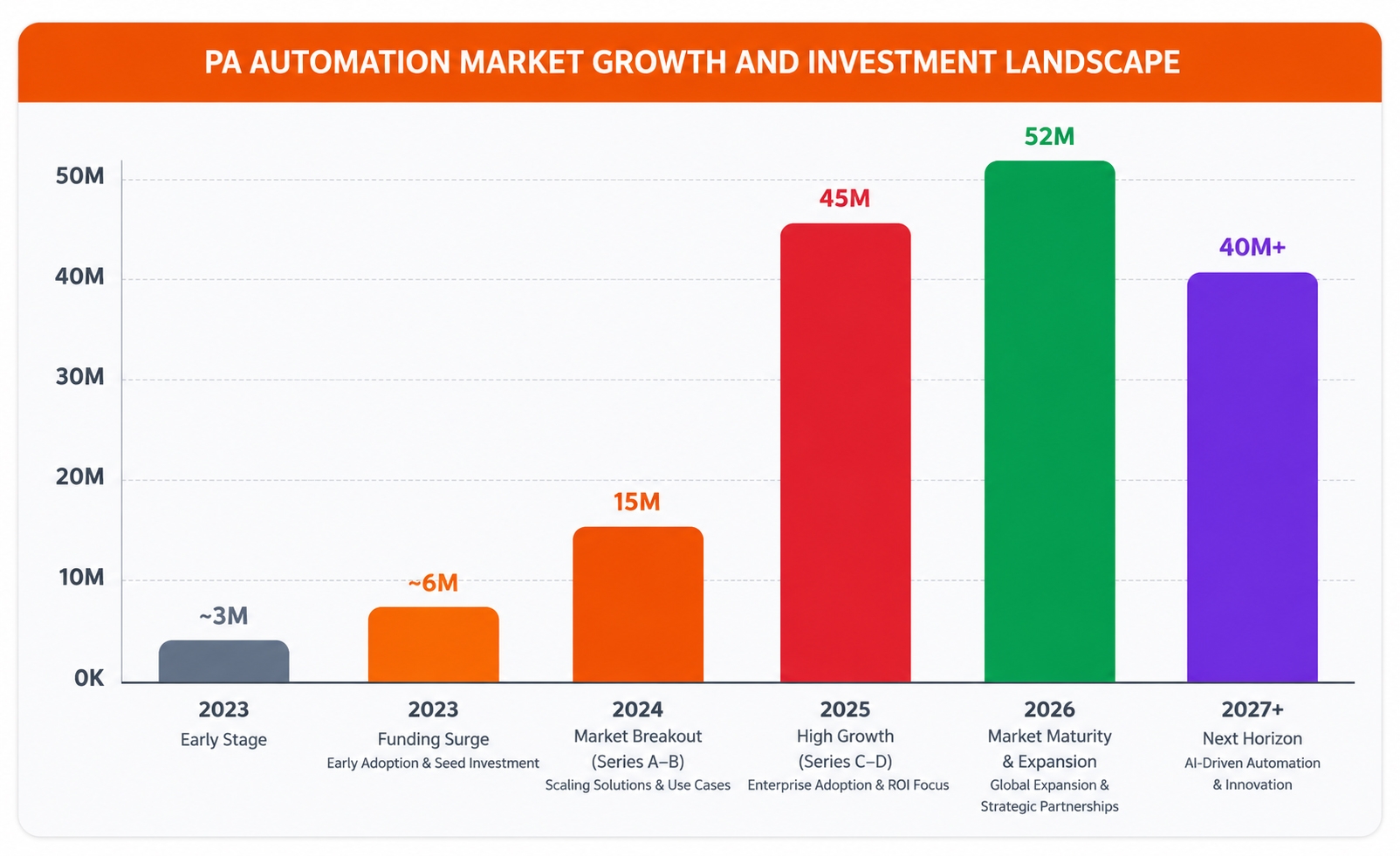
The question for healthcare product companies and digital health engineering teams today isn't whether to address this problem. It's whether they can move fast enough. Investment in PA automation technology is growing at 10x year-over-year and the organizations that build or integrate intelligent automation now will define the next decade of healthcare operations.
Root cause analysis
Why Prior Authorization Became a Healthcare Software Engineering Problem
Prior authorization sounds like a business process problem. And it is. But its root cause is a healthcare software engineering challenge involving interoperability, workflow orchestration, and real-time data exchange. The industry built a massively complex payer-provider interaction on a foundation of faxes, PDFs, phone calls, and disconnected portals.
Each payer has its own submission requirements. Each insurance plan within a payer has its own coverage policies, which change frequently and are inconsistently documented. EHR systems don't talk to payer systems in real time, creating significant barriers for organizations building modern healthcare software products.
"According to MGMA's 2024 administrative burden report, practice spending on prior authorization staffing jumped 43% between 2019 and 2024, even as reimbursement lagged. The problem isn't clinical it's structural."
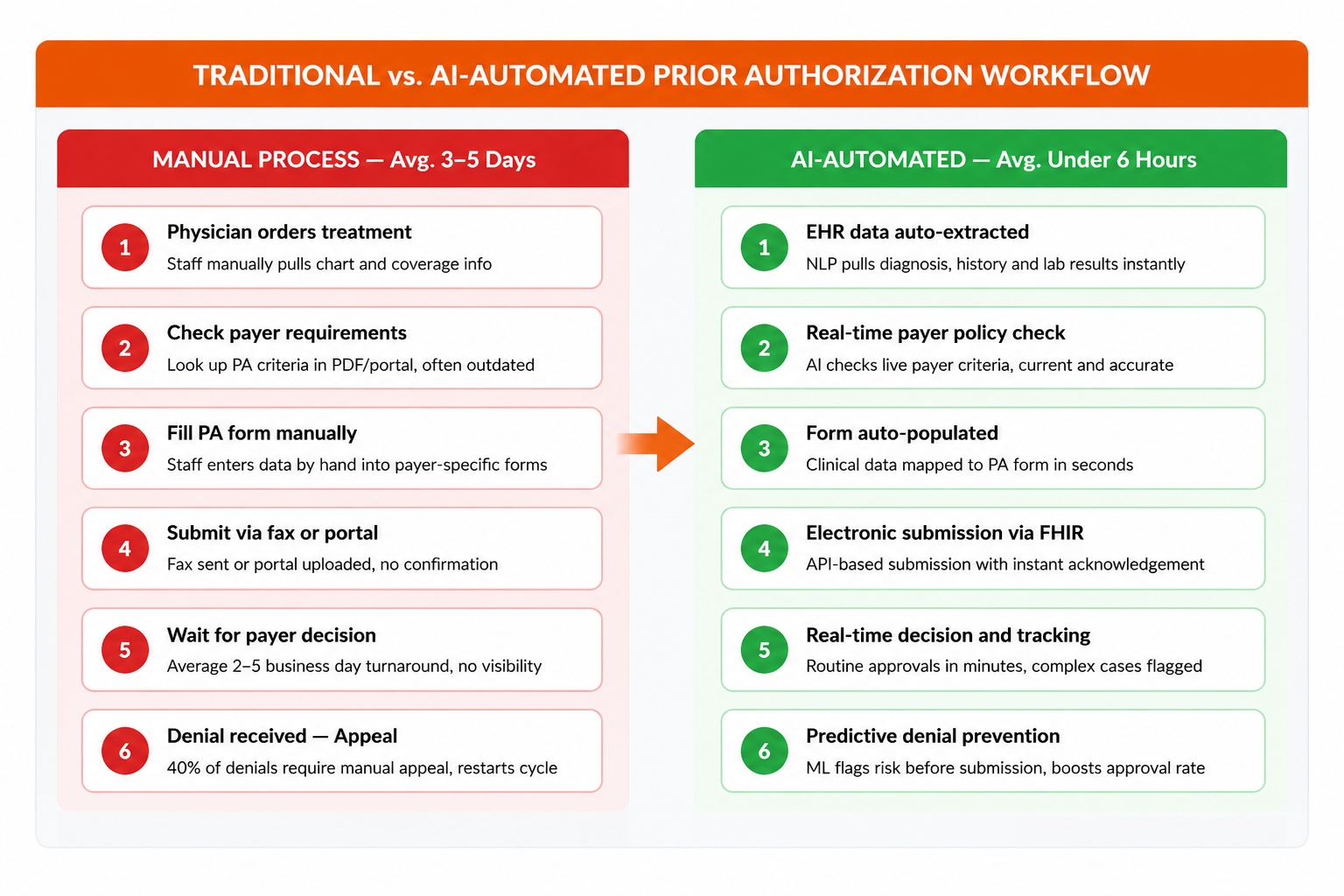
Traditional RPA tools offered a partial answer automating repetitive click-and-fill tasks within web portals. But RPA breaks when payer portals update their layouts. It can't interpret unstructured clinical documentation. It can't predict which requests are likely to be denied. RPA was a digital band-aid over a structural wound.
Engineering reality check
Why Most Healthcare Product Teams Underestimate PA Automation Complexity
PA automation appears straightforward at first glance. Many internal teams assume it is simply an integration project. In practice, platforms built with product engineering services succeed where internal efforts stall because they tackle five separate engineering challenges simultaneously:
1. EHR interoperability:
Extracting structured and unstructured clinical data from Epic, Cerner, Athena, and Meditech each with different APIs, data models, and access patterns.
2. Multi-payer connectivity:
A provider network may interact with dozens of payers, each with different submission systems, API support levels, and portal architectures.
3. Clinical NLP:
Parsing unstructured physician notes to extract diagnosis codes, lab results, treatment history, and clinical justifications at scale.
4. Workflow orchestration:
Routing submissions intelligently, tracking status in real time, and surfacing only the exceptions that require human review.
5. Compliance and auditability:
Building human-override mechanisms, explainability for ML models, and audit trails that satisfy growing state and federal regulatory requirements.
This complexity is why many internal PA automation initiatives stall after initial prototypes. Organizations that reach production consistently partner with teams that have already solved the integration layer.
Core positioning
PA Automation Is Not an AI Project. It Is a Product Engineering Challenge.
When AI/ML Development Services appear in PA automation headlines, it's easy to assume that model accuracy is the limiting factor. It rarely is. Successful platforms require a full stack of engineering capability working in concert:
Cloud-native, scalable microservices architecture
Secure EHR and payer integrations that don't break on platform updates
Workflow orchestration engines that handle exceptions gracefully
DevOps pipelines that support continuous compliance and rapid iteration
AI/ML models trained on payer-specific labeled data with governance built in
AI is only one layer of the solution. Without strong product architecture beneath it, even accurate models fail to deliver operational value. The organizations seeing the fastest PA automation ROI are not the ones who built the most sophisticated AI they are the ones who solved the integration layer first.
This is also where Agentic AI Development Services are beginning to play a significant role: not just predicting denial likelihood, but autonomously gathering supplemental documentation, routing to the right clinical reviewer, and triggering appeals workflows all without manual intervention for routine cases.
Capability breakdown
What Modern AI Prior Authorization Software Actually Does
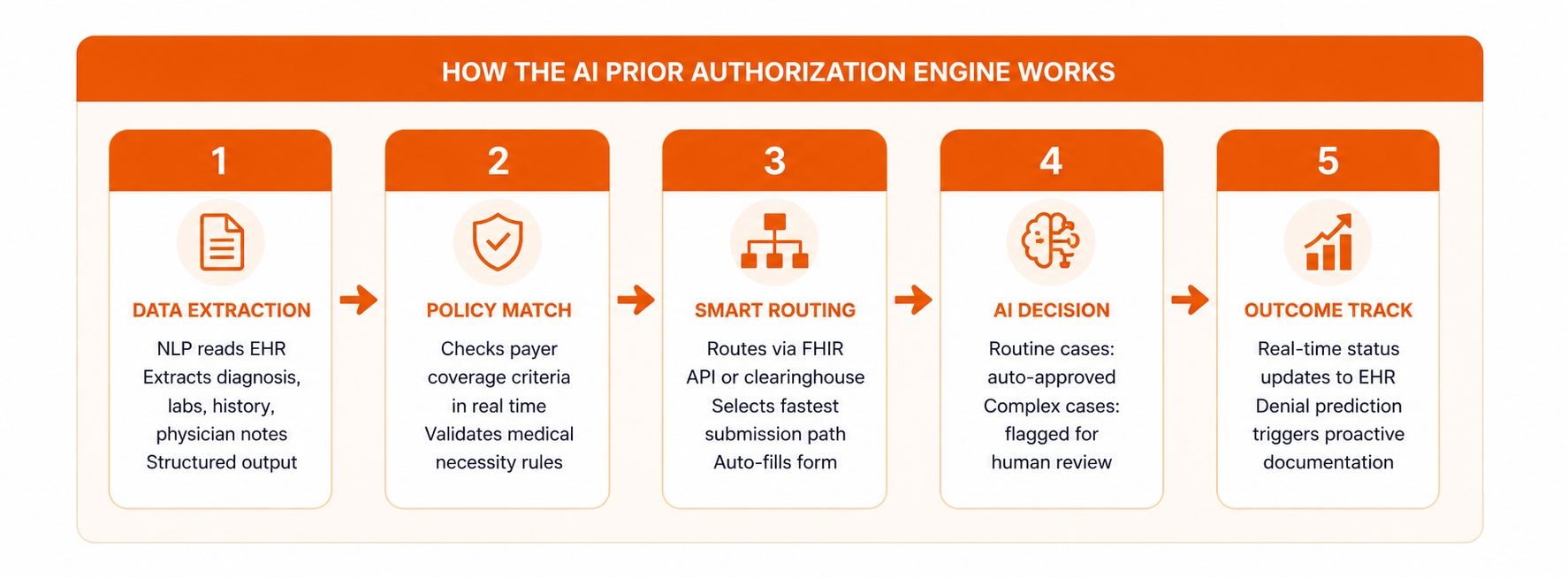
Modern AI-powered prior authorization software combines multiple technologies to streamline approvals while improving operational efficiency. Working together, these capabilities fundamentally change how authorization workflows operate.
1. Real-Time Payer Policy Intelligence
Instead of relying on static documentation, advanced healthcare automation platforms continuously ingest and parse payer coverage policies, formulary updates, and prior auth criteria. When a provider submits a request, the system already knows whether that service requires authorization for that specific plan and what evidence is required.
2. Automated Clinical Documentation Extraction
Using natural language processing (NLP) applied to EHR records, modern healthcare AI solutions extract relevant clinical data diagnosis codes, lab results, treatment history, physician notes and auto-populate authorization forms. What previously required 20–40 minutes of staff time per case becomes a near-instant operation.
3. Intelligent Submission Routing and Status Tracking
Rather than submitting through payer-specific portals manually, automated systems route submissions electronically via FHIR APIs where available, and through optimized clearinghouse connections where not. Status tracking happens in real time, with exception alerts surfacing only the cases that genuinely require human review.
4. Predictive Denial Prevention
Machine learning models trained on historical payer decision data can predict, with increasing accuracy, which PA submissions are likely to be denied and why. Armed with this signal, clinical staff can proactively supplement documentation before submission, significantly improving first-pass approval rates.
5. Human-in-the-Loop for Complex Cases
Mature PA automation is designed to handle high-volume, straightforward requests automatically while surfacing complex, borderline, or high-risk cases to experienced staff for clinical judgment. This is the architecture that wins regulatory approval and clinician trust simultaneously.
Impact metrics
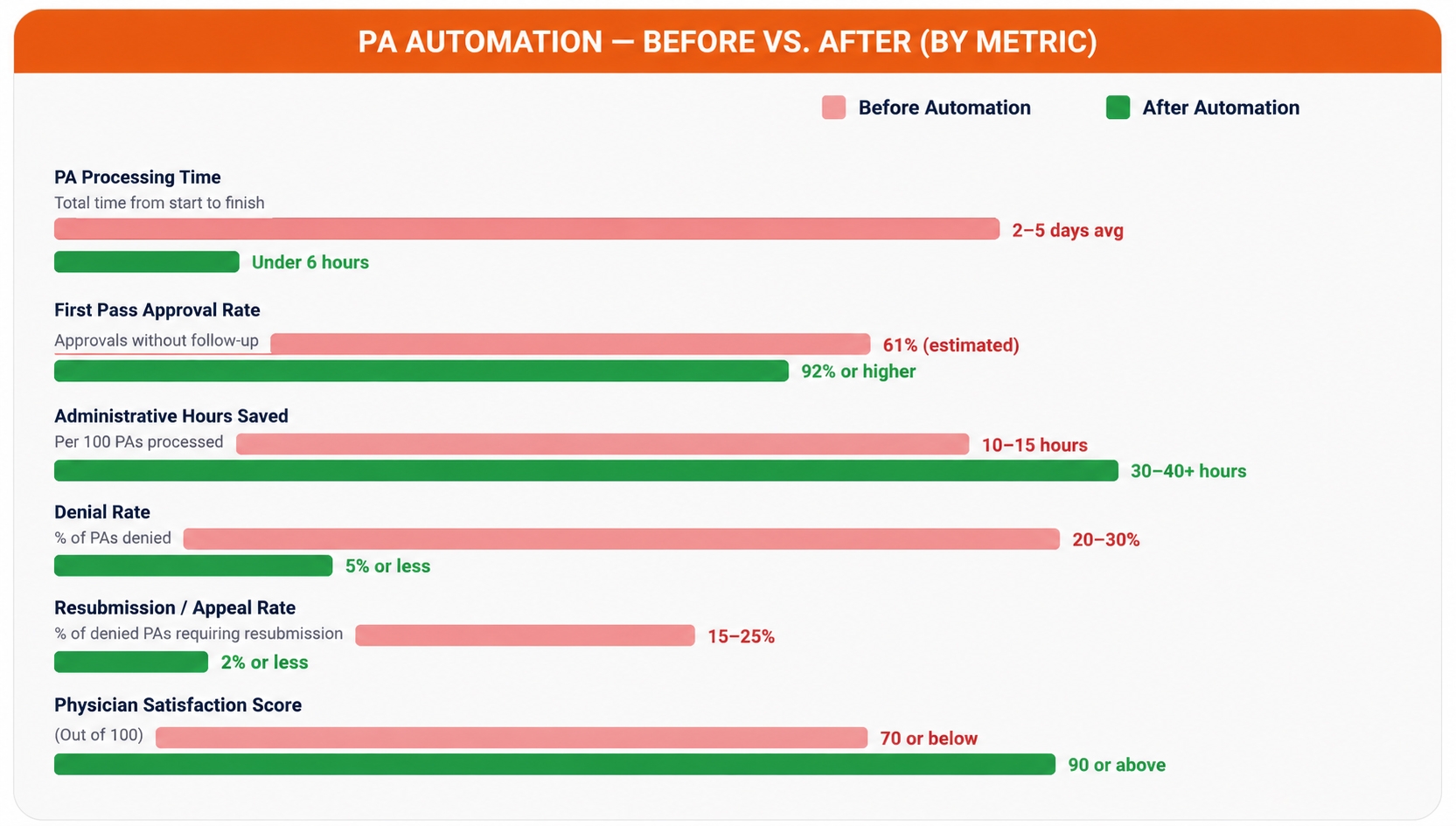
Before and After: What the Numbers Show
Technical architecture
The Engineering Architecture Behind PA Automation
For engineering leaders building or evaluating PA automation, the technical architecture involves several interconnected components. FHIR integration and healthcare API integration sit at the center of everything without them, real-time payer connectivity and EHR data extraction remain out of reach.
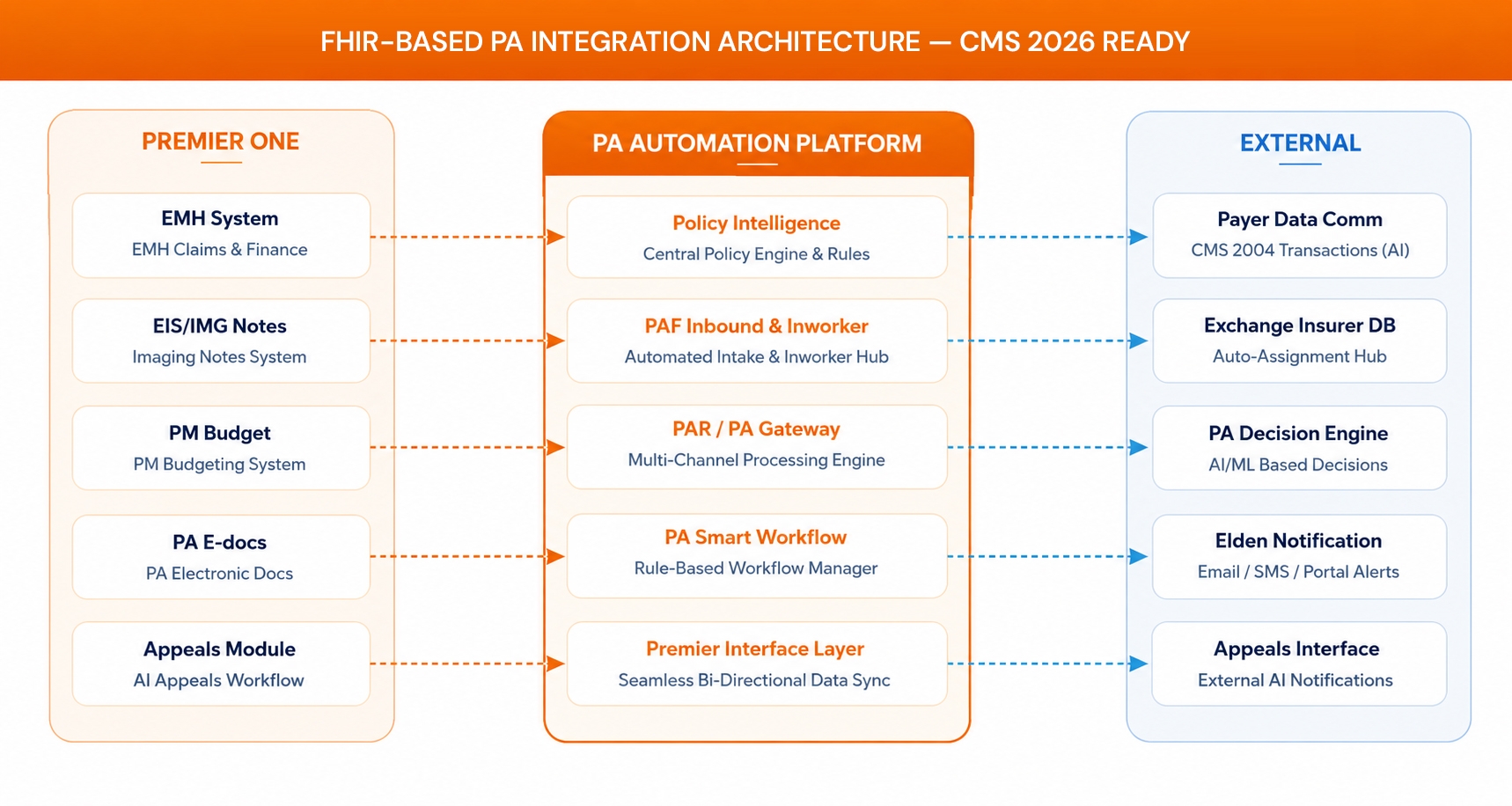
EHR Integration via FHIR APIs
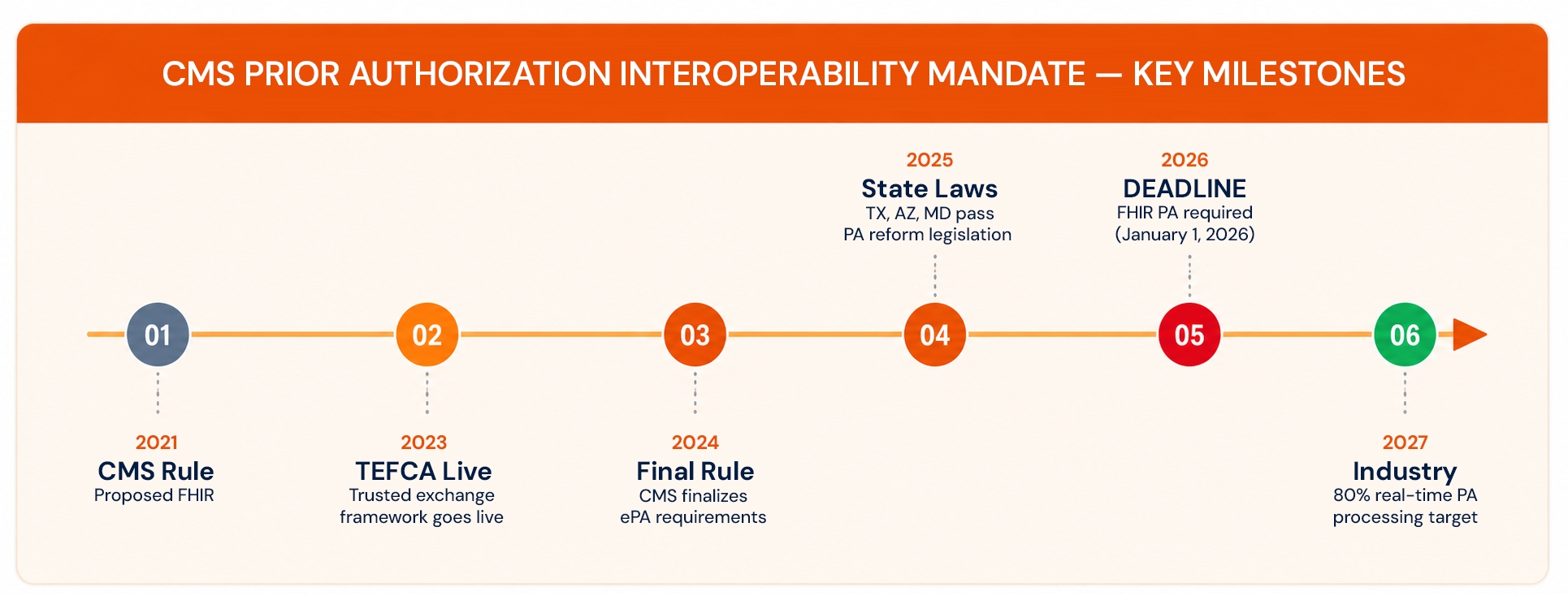
The move toward HL7 FHIR R4 as the interoperability standard is reshaping what's possible for FHIR integration, healthcare API integration, and electronic prior authorization workflows. CMS's 2026 prior authorization interoperability mandate requires payers to implement FHIR-based APIs for PA submissions which means product teams building on FHIR now will have a structural advantage when that deadline arrives.
Payer Connectivity at Scale
A provider network may interact with dozens of different payers, each with different submission systems, API support levels, and portal architectures. Building and maintaining those connections in-house is expensive and fragile, especially for organizations developing enterprise healthcare software platforms. The strongest architectures use clearinghouse partnerships or abstraction layers that normalize payer variability behind a single integration interface.
ML Model Training and Governance
Predictive denial models require labeled historical data, which is payer-specific and volume-dependent. Model governance explainability, bias auditing, human override mechanisms is also a growing regulatory requirement as states expand PA oversight.
Regulatory timeline
The CMS 2026 Mandate: What Engineering Teams Need to Know
Market context
The Business Case Is No Longer Theoretical
Menlo Ventures' 2025 State of AI in Healthcare report placed administrative services in front-office RCM at $98 billion in annual spend, with software penetration at just 3%. For mid-market healthcare product companies investing in healthcare product development, the strategic imperative is clear: PA automation is transitioning from a differentiator to a baseline expectation.
Strategic decision framework
Build, Buy, or Engineering Partnership?
Most mid-market healthcare product companies arrive at this decision after an internal proof-of-concept stalls. Here's an honest comparison of the three paths:
| Approach | Pros | Cons | Best Fit |
|---|---|---|---|
| Buy SaaS | Fast implementation; predictable cost structure | Limited customization; potential vendor lock-in | Point solutions with low workflow complexity |
| Build Internal | Full control over roadmap and architecture; IP ownership | High development cost; longer timeline; staffing and maintenance risk | Large health systems with dedicated engineering organizations |
| Engineering Partnership | Faster delivery with flexibility; proven healthcare integrations; compliance expertise built in | Requires governance alignment and onboarding investment | Mid-market healthcare product companies building for scale |
The organizations seeing the fastest PA automation ROI are those that solve the integration layer first, then layer AI sophistication on top of a proven foundation.
Where partners add value
Where Engineering Partners Add the Most Value
Successful initiatives often require a combination of product engineering services, healthcare software development, AI expertise, and cloud-native architecture. Building PA automation from scratch is not the right move for most mid-market healthcare product companies. The highest-value engineering engagements in this space tend to focus on:
FHIR API integration and healthcare interoperability with existing EHR systems (Epic, Cerner, Athena, Meditech)
Building configurable rule engines for payer-specific PA criteria
Developing NLP pipelines for unstructured clinical note extraction
Creating auditability and human-override mechanisms for regulatory compliance
Designing scalable microservices architectures for multi-payer connectivity
Conclusion
The Window for Strategic Action Is Now
Prior authorization has been a known problem for decades. What's changed is the engineering toolkit available to solve it and the regulatory pressure accelerating adoption. FHIR APIs are maturing. NLP models can parse clinical documentation with increased accuracy. Payer connectivity platforms are reducing the integration surface area. And the business case, once murky, is now measurable.
For mid-market healthcare product companies, successful prior authorization automation requires more than AI. It depends on strong product engineering, scalable cloud architecture, secure integrations, and reliable healthcare software delivery. The organizations building these capabilities now will be the ones positioned to lead as the 2026 mandate reshapes the market.
The strategic question is not "Should we build PA automation?" It's "How quickly can we architect and deploy it, and who are the right engineering partners to accelerate that timeline?"
Frequently Asked Questions
What's the difference between electronic prior authorization (ePA) and AI-driven PA automation?
ePA refers broadly to digitizing the PA submission process moving from fax and phone to electronic forms and portals. AI-driven automation goes several layers deeper: it extracts clinical data from EHRs automatically, checks payer criteria in real time, predicts denial likelihood, and routes cases intelligently. ePA is the foundation; AI automation is the acceleration layer on top.
Is fully automated PA approval possible, or does human review always apply?
Fully automated approvals are possible for routine, low-risk cases where clinical evidence clearly meets payer criteria. However, several states now require clinician review before any adverse determination meaning fully automated denials are legally prohibited in a growing number of jurisdictions.
What ROI should healthcare product companies expect from PA automation?
Well-implemented platforms consistently show: PA processing time reduced from 3–5 days to under 6 hours for routine cases, staff time on PA reduced by 60–70%, first-pass approval rates improved from ~70% to 85–90%, and PA staff costs reduced by up to 85% for automated case subsets (Highmark Health, 2024).
What are the biggest implementation risks?
The most common failure modes are: (1) underestimating payer connectivity complexity, (2) treating it as an AI project rather than an integration project, (3) insufficient labeled historical data for denial prediction models, and (4) compliance architecture added as an afterthought rather than designed in from the start.
How does the CMS 2026 PA interoperability mandate affect our product roadmap?
If your product serves Medicare Advantage, Medicaid, or CHIP payers, the January 2026 CMS mandate requires FHIR-based PA APIs. Building on FHIR now is solving for compliance and competitive advantage simultaneously.
What's the realistic implementation timeline for a mid-market healthcare product company?
A focused implementation covering EHR integration, payer connectivity for the top 5–10 payers, and basic workflow automation typically takes 3–6 months. Adding predictive analytics and ML-driven denial prevention layers an additional 2–4 months. Total timeline to a production-grade platform: 5–10 months with the right engineering partner.
How do we handle multi-payer environments without building a separate integration for each?
The standard approach is to use a clearinghouse intermediary or an abstraction layer that normalizes payer-specific differences behind a unified API. Vendors like Availity and Change Healthcare (now Optum) handle payer translation at scale.
Ready to Scale Prior Authorization Automation?



