







The Real Problem Starts Before the First Line of Code
Hospitals invest heavily in digital tools, yet patient adherence rates remain stubbornly low. The uncomfortable truth? Most patient engagement platforms fail not because of bad technology they fail because the wrong problems are being solved first.
A platform built around features instead of patient behavior will always underperform. Before your team writes a single line of code or signs a vendor contract, the foundational question must be: are we solving a clinical problem or building a digital brochure?
This blog is written for hospital operators, healthtech founders, and product leaders who are evaluating, building, or scaling patient-facing platforms. If you've already launched something and aren't seeing adherence move or no-show rates haven't budged this is especially for you.
What Is a Patient Engagement Platform?
A patient engagement platform is a digital system that helps patients follow their care plans through structured reminders, secure communication, behavioral interventions, and real-time health tracking. Its core purpose is to reduce the gap between clinical recommendations and actual patient behavior improving adherence, reducing no-shows, and driving measurable clinical outcomes.
Done right, patient engagement platform development connects EHR data, wearable inputs, and patient-facing interfaces into one cohesive system that care teams can monitor and act on. Done wrong, it becomes an expensive notification tool that patients ignore within 30 days of onboarding.
The Scale of the Problem Why This Matters in the US
According to WHO estimates, patient non-adherence costs the global healthcare system over $1 trillion annually. The CDC reports that more than 60% of US adults live with at least one chronic condition. In that context, patient engagement solutions healthcare providers deploy aren't optional infrastructure they are clinical risk management tools.
A study from NEJM Catalyst found that digital health engagement platforms achieving 20–30% adherence improvement correlated with 15% better clinical outcomes, including meaningful HbA1c reductions in diabetes management cohorts.
Key Insight: The platforms that move adherence aren't the ones with the most features they're the ones with the clearest behavioral pathways built into the product experience.
The Metrics That Separate High-Performing Platforms From the Rest
Too many platform teams optimize for logins and session counts. The metrics that actually drive outcomes in patient engagement solutions look very different.
| Metric | Typical Baseline | Target With Right Platform Design |
|---|---|---|
| Medication Adherence Rate | ~50% | 75–85% |
| Appointment No-Show Rate | 20–30% | Below 10% |
| 30-Day Readmission Rate | 15–20% | Below 12% |
| Patient Satisfaction (NPS) | 60–70 | 85+ |
| Daily Active Usage (DAU) | 10–15% | 30%+ |
If your platform is already live and these numbers haven't moved within 90 days, the problem is almost never a missing feature it's a design or integration gap that compounds over time.
Where Most Platforms Break Down What Leaders Rarely Hear
Here is what decision-makers rarely hear from their tech teams during build: the biggest failure risks are not architectural they are behavioral and organizational. The three most consistent failure patterns across patient engagement software implementations are feature overload at launch, integration complexity that is severely underestimated, and a complete absence of behavioral design.
Feature overload is the most common early mistake. Teams build dashboards, reminders, video consult, health logs, and gamification all at once. Patients open the app once, feel overwhelmed, and never return. How to improve patient adherence starts not by giving patients more tools it starts by removing every obstacle between them and the single most important action in their care plan.
Most EHR integrations take 2–4 months not 2 weeks as commonly assumed. Connecting to Epic or Cerner via FHIR APIs requires environment configuration, data mapping negotiations, and multiple testing cycles that most project timelines don't account for. This is consistently where budgets and timelines slip.
The third failure and the most invisible is the absence of a behavioral design layer. Reminders fire at fixed times. Nudges are generic. Nothing adapts based on what a patient actually does or doesn't do. Reduce hospital no-shows software alone won't work if the communication logic doesn't account for patient behavior patterns over time.
Key Insight: If your platform already has low adoption, the problem is almost always UX and behavioral design not the number of features or reminders being sent.
Build vs. Buy What Most Teams Get Wrong
This is one of the most searched questions among leaders evaluating digital patient engagement investments, and most teams answer it based on speed rather than fit.
| Option | When It Works Best | Primary Risk |
|---|---|---|
| Build custom | >10K patients, complex workflows, strong internal product team | Scope creep, timeline overrun without structured Product Strategy & Consulting |
| Buy white-label | Faster time-to-market, standardized care workflows | Limited behavioral customization, integration constraints |
| Hybrid (buy core, build layer) | Mid-size networks needing flexibility | Integration complexity between vendor platform and custom layer |
| Delay entirely | <5K patients, unstandardized workflows | None premature build is a common and costly mistake |
One point that doesn't get said often enough: if you have fewer than 5,000 active patients or your clinical workflows are not yet standardized, you should delay the build. The platform will not generate ROI at that scale, and the complexity will consume resources that are better spent on workflow standardization first.
When You Should NOT Build a Patient Engagement Platform
This section builds more trust than any feature list. There are real scenarios where building is the wrong answer and recognizing them early saves significant cost:
Workflows are inconsistent across care teams. A platform cannot automate chaos it amplifies it.
No internal product or clinical informatics ownership. Without a clear internal owner, platforms drift toward feature accumulation rather than outcome improvement.
EHR data quality is poor. If the underlying patient data is incomplete or fragmented, engagement logic built on top of it will produce irrelevant interventions.
Patient volume is below 5,000. At this scale, the operational overhead of a custom platform rarely justifies the investment.
Approximate Cost Ranges What to Budget
Decision-makers always need directional numbers. Here is a realistic range based on platform scope for patient engagement platform development:
MVP (core dashboard, reminders, basic FHIR sync): $80K–$150K, delivered in 3–5 months
Mid-tier platform (behavioral nudges, analytics, provider dashboard, telehealth): $200K–$350K, 6–9 months
Full enterprise platform (AI personalization, multi-EHR integration, RPM, custom reporting): $400K–$650K+, 10–14 months
Integration cost as a % of total build: typically 25–35% of total budget the most underestimated line item
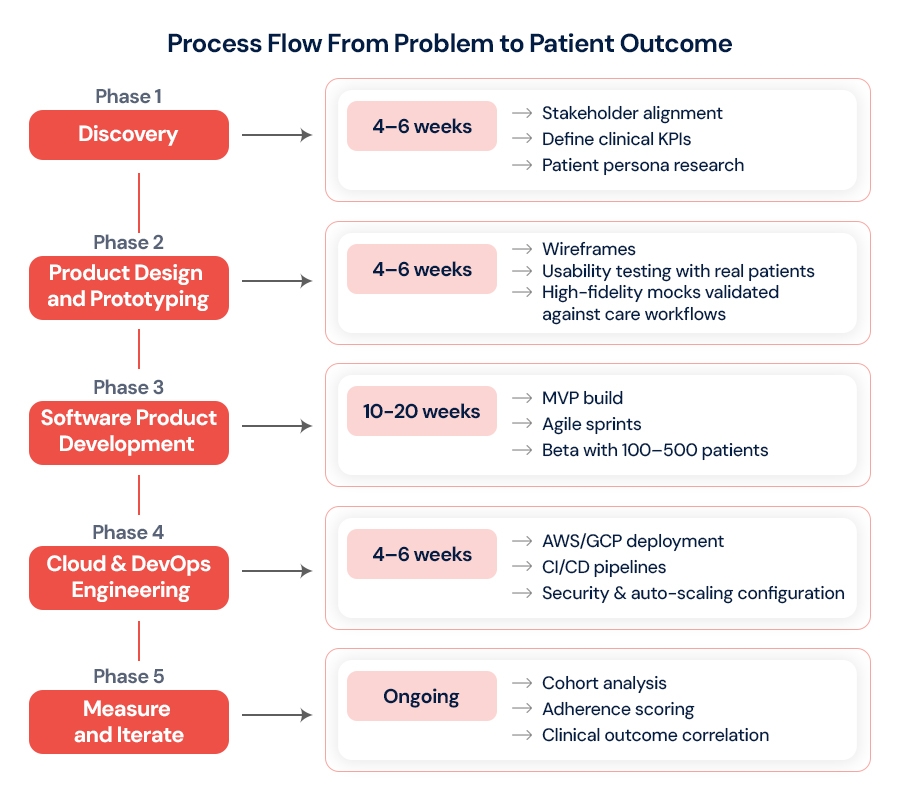
These ranges assume structured Software Product Development with agile delivery. Teams that skip discovery and go straight to build typically spend 40–60% more on post-launch rework.
The Architecture Decisions That Define Long-Term Cost
Healthcare patient engagement tools built on monolithic backends struggle to scale specific features independently. A microservices approach while more complex upfront allows you to scale the notification engine separately from the analytics layer, which is where most load concentrates as patient counts grow.
| Decision | Short-Term Impact | Long-Term Risk If Wrong |
|---|---|---|
| Monolith vs. Microservices | Faster early delivery | Cannot scale components independently |
| Managed cloud vs. self-hosted | Lower ops overhead | Cost spikes at 100K+ users |
| Custom FHIR connector vs. middleware | More control | Maintenance-heavy, EHR version-dependent |
| Rule-based alerts vs. ML-driven nudges | Simpler to build | Low personalization, lower engagement over time |
| Native app vs. PWA | Better UX | Higher dev cost, dual maintenance |
Cloud and DevOps Engineering decisions here are not optional refinements they are core product decisions. A well-designed CI/CD pipeline with container orchestration allows your team to push adherence model updates without downtime, which matters when interventions are tied to clinical schedules.
Teams that treat Product Design and Prototyping as a distinct phase not a compressed pre-development checkbox consistently report lower post-launch rework costs and faster adoption curves.
What Behavioral Science Tells Us That Technology Ignores
Improving patient adherence through technology requires understanding one core principle from behavioral economics: people respond to friction, not logic. Adding a reminder does not change behavior if the action being prompted feels complicated.
Reducing friction making it two taps to confirm medication taken rather than navigating three screen has a measurable impact. Platforms that implement choice architecture (for example, "Take now or set a new time?" instead of a generic alert) report 15–20% higher response rates on nudges.
The digital tools for patient adherence that consistently work include contextual nudges tied to wearable or activity data, progress streaks that build continuity incentives without heavy gamification infrastructure, simplified care plan language that explains the why behind each action, and peer benchmarking within specific cohorts particularly effective in chronic disease management.
A mid-sized US hospital network implementing these behavioral principles alongside custom FHIR connectors and serverless alert infrastructure saw adherence rise 28% and readmissions drop 18% within 12 months.
Key Insight: Reducing friction improves adherence more than increasing reminder frequency. One well-timed, context-aware nudge outperforms five generic push notifications every time.
What Good ROI Actually Looks Like
Patient engagement solutions for healthcare providers that deliver real ROI define success in clinical terms from Day 1. Platforms like Livongo report 2.5x ROI within 12 months at scale. The formula is straightforward:
ROI = (Cost Savings from Reduced Readmissions − Platform Cost) ÷ Platform Cost × 100
For a hospital system with 50,000 active patients, reducing 30-day readmission rates from 18% to 12% generates enough avoided cost to recover platform investment within 8–14 months. But this only holds if adoption is broad not concentrated in health-conscious early users. Sustainable patient engagement and care outcomes improvement requires consistent usage across full patient cohorts, not just engagement spikes at launch.
Common Questions Leaders Ask Before Building
Why do most patient engagement platforms fail?
Low adoption is the primary cause driven by poor UX, feature overload at launch, and generic communication that doesn't adapt to patient behavior.
How long does it take to build a patient engagement platform?
MVP in 3–5 months. Full platform in 6–9 months. EHR integration alone adds 2–4 months to any timeline.
What is the cost of patient engagement software development?
MVP: $80K–$150K. Full platform: $400K–$650K+. Integration typically adds 25–35% to total cost.
Build vs. buy which is better?
Depends on patient volume, workflow complexity, and customization needs. Below 5,000 patients, buying or delaying is almost always the right answer.
What is the ROI timeline?
Typically 8–14 months for platforms that achieve broad adoption and measurable readmission reduction. Partial adoption extends this significantly.
Quick Decision Guide What This Means for You Right Now
If you're building from scratch → Prioritize behavioral design and FHIR integration planning before any frontend development begins
If you're buying a platform → Validate integration complexity with your EHR vendor before signing don't assume standard connectors work out of the box
If adoption is already low → Audit the onboarding flow and notification logic first, not the feature roadmap
If ROI isn't showing within 6 months → Measure readmission reduction and no-show rates, not logins
Teams we work with typically discover 2–3 significant gaps in their first platform audit gaps that were invisible during the build phase but become costly at scale.
What's Coming And Why Your Decisions Today Matter
The next 24 months will shift the patient engagement strategies in healthcare landscape meaningfully. AI health agents will move from notification systems to genuine care coaching conversational, context-aware, and personalized beyond what rule engines can achieve today. Federated learning will allow adherence prediction models to train across patient populations without centralizing sensitive data, solving the privacy challenge that blocks many providers currently.
None of this is a reason to wait. The providers building solid foundational platforms now with clean data architecture, strong EHR integration, and behavioral design will layer these capabilities in without rebuilding from scratch. The providers who wait will pay twice: once to build, and again to fix.
Closing: Build for Behavior, Not Features
The platforms that consistently improve care adherence and reduce no-shows share one quality: they were designed around what patients actually do, not what clinicians assume they will do. That requires structured Product Strategy & Consulting before development begins, behavioral science thinking alongside engineering, and a clear definition of clinical success before the first sprint starts.
If your organization is evaluating where to start or where things went wrong the most valuable next step is an honest platform review with people who have seen what works at scale and what doesn't.
AspireSoftserv's product engineering services team works with hospital systems and healthtech founders across the US to design, build, and scale patient engagement platforms built for real-world adoption. Whether you're starting fresh or fixing what's already live, we help you close the gap between platform investment and clinical outcome.
Reduce no-shows with smarter engagement




