







The Revenue Leak That Most Hospitals Can't See Until It's Too Late
Every year, U.S. healthcare providers lose up to $265 billion to claim denials and medical billing errors not because of bad medicine, but because of broken systems. The average mid-sized hospital absorbs $11.3 million annually from preventable billing failures. That's not a rounding error. That's a structural crack running through the foundation of your revenue cycle.
What makes this particularly costly is what happens after a denial. A denied claim doesn't just delay payment it triggers rework cycles, administrative burnout, compliance exposure, and in many cases, permanent write-offs. 15–20% of denied claims are never resubmitted resulting in permanent, unrecoverable revenue loss. For a hospital processing $100M in annual billing, a 12% denial rate puts $12M at risk every year and $24M+ over two years if the architecture gap goes unaddressed.
For CTOs and operations leaders, this is both a financial and an engineering problem. And like most engineering problems, it has a solvable architecture if you know where to look.
Most teams don't realize this until they map their denial patterns something we typically uncover in the first audit.
💡 Why Are Healthcare Claims Rejected? Quick Answer
Healthcare claims are most commonly rejected due to front-end errors: incorrect patient data, eligibility verification failures, missing documentation, and coding mismatches. In most cases, these errors occur before submission and are not caught because legacy systems lack real-time validation. 60–70% of claim denials originate at the front end during registration and pre-authorization not in the billing or coding team.
What Is Revenue Cycle Management (RCM)?
Revenue Cycle Management (RCM) is the end-to-end process of managing patient revenue from registration and eligibility verification through claims submission, denial management, and final payment posting. It is the financial backbone of every healthcare organization, and when it breaks down, the impact is felt across operations, cash flow, and patient experience simultaneously.
For most hospitals and health systems, RCM is where clinical excellence meets operational reality. A well-engineered revenue cycle management system ensures that every dollar of care delivered is accurately captured, correctly billed, and efficiently collected. A poorly built one silently hemorrhages revenue at every step and most organizations don't see the full scale of the loss until they run their first structured audit.
Where Healthcare Revenue Is Lost in Claims Processing
Most healthcare leaders assume denials are a back-office problem something the billing team resolves after the fact. The data tells a different story. The majority of healthcare claims processing failures originate at the very beginning: patient registration, eligibility verification, and pre-authorization. By the time a claim reaches the payer, the error has already been embedded.
Here's what the numbers reveal:
| Error Type | Prevalence | Avg. Denial Rate | Financial Impact per 1,000 Claims |
|---|---|---|---|
| Wrong CPT / medical billing errors | 29% | 15% | $118,000 |
| Eligibility verification gaps | 17% | 12% | $72,000 |
| Missing documents / timely filing | 14% | 10% | $60,000 |
| ICD-10 coding mismatches | 12% | 18% | $108,000 |
| Duplicate submissions | 8% | 5% | $30,000 |
Source: Adapted from MGMA 2025 Benchmarks
Each of these failures compounds. A single denied claim costs $25 to rework on average. Appeals processed manually average 80 days to resolve, aging AR well past the 45-day threshold most CFOs consider acceptable. This isn't a 10–15% inefficiency. It's a 3–5x operational drag that compounds every quarter and most of it is preventable with the right system design.
Why Healthcare Claims Get Rejected: It's a Design Limitation, Not a People Problem
Why healthcare claims get rejected is a question most providers answer incorrectly. They blame coders, billers, or payer complexity. The honest answer is more structural: legacy revenue cycle management systems were never designed to validate claims in real time. They were built for batch processing in an era when volumes were predictable and payer rules changed slowly. Neither condition exists today.
Post-pandemic, claim volumes surged by 25% (Change Healthcare). Payer policies shifted faster than static rule engines could track. The result is a linear, batch-driven process with no feedback loop and no mechanism to catch problems before submission.
Legacy Claims Flow Where Errors Compound
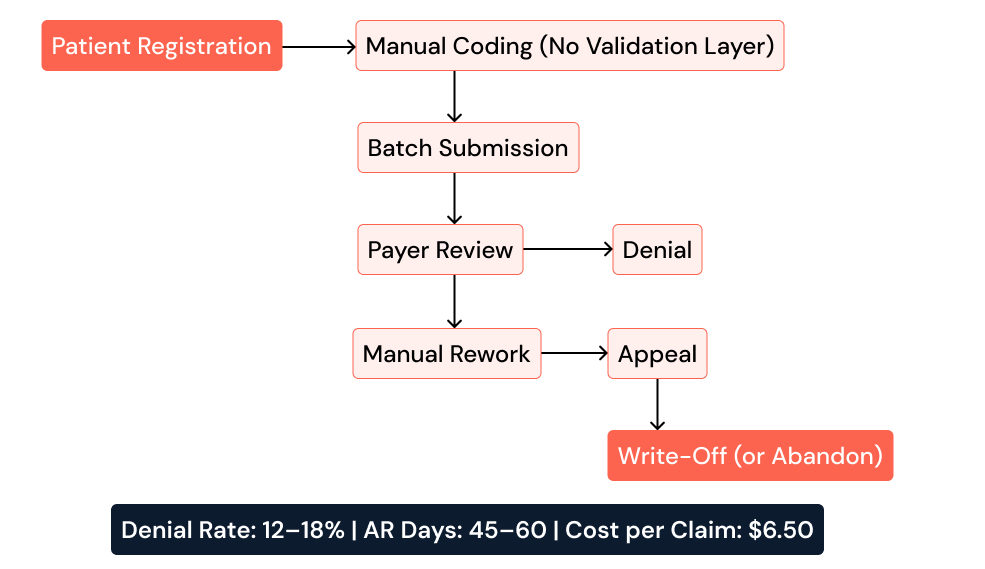
The core technical gaps driving this are consistent across legacy environments:
Integration failures between EHRs like Epic and RCM platforms create data silos, contributing to a 30% increase in denial rates
Static rule engines cannot adapt to payer variability, producing an 18% rework rate
Monolithic architecture collapses under volume spikes, adding 45-day AR delays during peak periods
No real-time eligibility validation means front-end errors pass through undetected until the payer rejects them
Common Mistakes That Keep Denial Rates Stubbornly High
Before exploring solutions, it's worth naming the patterns that keep most organizations stuck. These are not rare oversights they are systematic errors repeated across health systems of every size:
Automating without fixing the root cause. Layering automation on a broken process doesn't eliminate denials it accelerates them at scale.
Over-reliance on manual audits. Periodic audits catch historical errors. They don't prevent future ones.
Ignoring front-end validation. Most denial reduction efforts focus on coding and appeals, while the majority of errors originate at registration.
Treating RCM as an operations problem, not an engineering one. When RCM is managed through spreadsheets and manual workflows, systemic improvement is structurally impossible.
Measuring denial rate without tracking denial reason by payer. Knowing your rate is 12% tells you nothing about where to intervene first.
Eighty percent of claim denials are preventable but only if the system is designed to prevent them, not just respond to them.
When Should You Fix Your RCM System?
Decision-makers often ask the right question too late: When is the right time to act? The answer is almost always: before the losses compound further. Specific triggers that indicate your system has reached an architectural breaking point include:
Denial rate consistently above 8% with no downward trend quarter-over-quarter
AR days increasing QoQ even with stable claim volume
Appeals taking more than 30 days to process and resolve
New payer integrations taking more than two weeks to go live
Eligibility errors appearing after claim submission rather than at registration
Billing team spending more than 20% of their time on rework rather than new submissions
If three or more of these apply to your organization, the issue is not operational it is architectural. And architectural problems require engineering solutions, not additional headcount.
How to Reduce Claim Denials in Healthcare: The Engineering Path
How to reduce claim denials in healthcare is not a staffing or training question. It is a product engineering question. The organizations recovering the most revenue are not hiring more billers they are rebuilding the system, layer by layer, with automation and AI embedded at every stage.
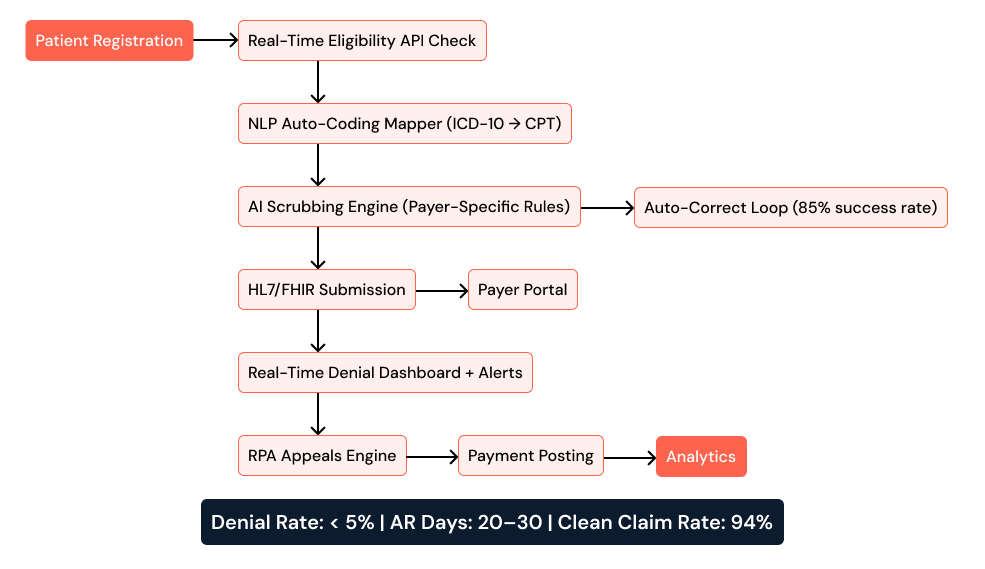
Pre-Submission AI Scrubbing AI-powered validation engines run payer-specific edits before a claim leaves the system cutting submission errors by up to 70% within the first 90 days. Unlike static rules, these models update continuously as payer policies shift, addressing one of the most persistent gaps in traditional revenue cycle management healthcare operations.
Real-Time Eligibility Verification Instead of overnight batch checks, modern platforms query payers in real time at the point of registration. This eliminates the single largest category of front-end denials: submitting claims for patients whose coverage has lapsed or changed since their last visit.
NLP-Driven Appeals Automation When denials occur, NLP models extract the denial reason, match it to the correct appeal template, and generate a response compressing appeal cycles from weeks to hours. Organizations using this approach consistently report appeal win rates above 78%.
Closed-Loop Analytics and Feedback Every denial feeds back into the rule engine, improving future submission accuracy. Dashboards surface medical claims errors by payer, by provider, and by claim type giving operations leaders the visibility to act before patterns become compounding revenue losses.
Modern RCM Flow AI-Enabled, Closed Loop
How to Improve Claims Processing Through Product Engineering
How to improve claims processing in healthcare requires more than new software. It requires intentional product architecture built through a disciplined engineering process one that addresses the problem at every layer, not just the most visible one.
Step 1: Identify Where Revenue Is Leaking
Product Strategy & Consulting begins by auditing the existing RCM stack mapping denial patterns by payer, provider, and claim type, and surfacing integration gaps between EHR and billing systems. This phase defines measurable success criteria like clean claim rate targets above 95%, and establishes a baseline before a single line of code is written. It also prevents the most expensive mistake in RCM modernization: automating a broken process instead of correcting it first.
Step 2: Design Workflows Around Real Operations
Product Design and Prototyping translates audit findings into denial heatmap dashboards, payer-specific rule interfaces, and workflow visualizations tested directly with billing and operations teams before development begins. For front-line staff, this means the platform reflects how they actually work. Adoption is faster, errors are fewer, and the feedback loop between clinical operations and the technical system becomes structural rather than incidental.
Step 3: Build Modular, Intelligent Claims Systems
Software Product Development delivers the core platform: AI scrubbers built in Python and TensorFlow, microservices for independent claims processing components, and HL7/FHIR-compliant submission engines. Because each module is independently deployable, updates to payer rules don't require system-wide releases or scheduled downtime a critical advantage in an environment where payer policies shift frequently.
Step 4: Enable Continuous Updates Without Disruption
Cloud and DevOps Engineering handles infrastructure Kubernetes for elastic scaling, Docker and Helm for zero-downtime deployments, and CI/CD pipelines that push payer rule updates into production within hours, not weeks. The result is 99.99% uptime during peak claim volumes the exact moments when system failures are most costly and most visible to leadership.
What This Looks Like in Practice
A 500-bed regional hospital approached AspireSoftserv with a 15% denial rate and $4.2 million in annual revenue loss. The root causes were straightforward: manual eligibility checks, a scrubbing engine last updated 18 months prior, and an appeals process running entirely through spreadsheets.
The engineering intervention followed the four-step framework above beginning with a Product Strategy & Consulting audit, moving through Product Design and Prototyping, phased Software Product Development, and deployment on cloud-native infrastructure with full Cloud and DevOps Engineering automation.
Results 12 months post-implementation:
Denial rate dropped from 15% to 5.7%
Clean claim rate improved from 72% to 94%
AR days reduced from 58 to 27
Annual revenue recovered: $3.1 million
ROI achieved: 4x in Year 1
The technology didn't disrupt clinical workflows. It changed the system underneath eliminating the structural friction that had been bleeding revenue every single month, invisibly.
Results vary based on system maturity, but most organizations identify 20–30% recoverable revenue in the first audit.
Legacy vs. Modern Revenue Cycle Management Systems: Key Differences
| Performance Metric | Legacy System | Engineered Platform |
|---|---|---|
| Denial Rate | 12–18% | < 5% |
| AR Days | 45–60 | 20–30 |
| Cost per Claim | $6.50 | $2.10 |
| Clean Claim Rate | ~72% | > 94% |
| Appeal Win Rate | 45–55% | > 75% |
| Scalability | Fixed capacity | Auto-scaling |
| Payer Rule Update Speed | Weeks | Hours |
Source: KLAS Research + Internal Benchmark Data
This isn't a marginal improvement. It's a 3–5x efficiency gap that directly impacts cash flow, operational overhead, and the long-term financial health of the organization. Most organizations that make this shift recover the engineering investment within the first year and continue compounding gains as the platform learns and improves.

Quick RCM Health Check 2-Minute Self-Assessment
Before investing in modernization, benchmark where you stand today. Answer these five questions:
What is your current first-pass denial rate? (Benchmark: < 6% for top-quartile systems)
Do you validate patient eligibility in real time at registration or overnight in batches?
Can you track denial reasons by individual payer from a single dashboard?
How long does your average appeal cycle take from denial to resolution?
How quickly can your team deploy a payer rule update when a policy changes?
If your answers reveal denial rates above 8%, eligibility checks running overnight, appeal cycles exceeding 30 days, or rule updates taking more than a week your system has a design limitation that point-solutions cannot fix. A structured engineering intervention is the logical next step.
Frequently Asked Questions
Why are healthcare claims denied most often?
The most common causes are eligibility verification failures, incorrect or mismatched CPT and ICD-10 codes, missing documentation, and payer rule non-compliance. Critically, 60–70% of these errors originate at the front end during registration and pre-authorization not in the billing or coding team.
What is a good denial rate for a healthcare organization?
Top-quartile healthcare systems maintain first-pass denial rates below 6%. Engineered RCM platforms consistently achieve denial rates below 5%. If your organization's rate exceeds 8%, systemic intervention is warranted not incremental process improvement.
How long does it take to reduce claim denials with a modern platform?
Most organizations using AI-powered scrubbing and real-time eligibility verification see measurable denial reduction within the first 90 days. Full system optimization including appeals automation and closed-loop analytics typically delivers peak performance within 6–12 months.
What causes front-end claims processing errors in healthcare?
Front-end claims processing errors healthcare teams encounter most often stem from manual patient data entry, lack of real-time eligibility API integration, missing pre-authorization workflows, and EHR systems that don't sync with RCM platforms. These gaps account for the majority of rejections that reach the payer.
Can automation alone fix a high denial rate?
No. Automation applied to a broken process accelerates errors at scale. Effective denial reduction requires fixing root-cause workflows first through Product Strategy & Consulting then layering automation on a corrected, validated foundation.
What Should You Do Next?
For organizations ready to move from diagnosis to action, the path forward is clear:
Benchmark your denial rate against industry standard top-quartile systems operate below 6%
Identify your top 3 denial causes by payer and claim type using your current data
Evaluate whether your system supports real-time validation at the point of registration
Assess your appeals cycle time anything above 30 days indicates a process that can be automated
Decide whether to optimize or rebuild based on the audit findings, some systems benefit from targeted fixes; others require a platform-level overhaul
Most organizations identify 20–30% recoverable revenue in the first structured audit. The question is not whether that revenue exists it's whether you have a system designed to capture it.
The Decision Most Leaders Delay Until It's Expensive
Medical claims errors above 8% and AR days above 40 are not inevitable. They are symptoms of systems built for a different era one where volumes were manageable, payer rules were stable, and manual processes were scalable. None of those conditions exist in 2025.
For technical leaders, the question is not whether to modernize. It is whether to act before losses compound further or after absorbing another 12–24 months of preventable denials, rework cycles, and write-offs that never appear on a single line item but show up clearly in margin erosion over time.
For a hospital processing $100M in annual billing, a 12% denial rate puts $12M at risk every year. Over two years, unaddressed, that's $24M+ in avoidable loss more than enough to fund a complete RCM platform transformation and deliver meaningful ROI within the first year.
The organizations recovering the most revenue right now are the ones that treated this as an engineering problem with an engineering solution built systematically, deployed reliably, and improved continuously. That shift in thinking is where the recovery begins.
AspireSoftserv delivers product engineering services purpose-built for healthcare organizations ready to rebuild their revenue cycle from the ground up. From Product Strategy & Consulting and Product Design and Prototyping through Software Product Development and Cloud and DevOps Engineering, our teams help providers recover revenue, reduce operational load, and build infrastructure that scales.
Reduce Claim Denials with Smarter RCM




